The OptiBreech Research and Public Involvement team share their work at the #BICS22 conference.
The OptiBreech Team enjoyed meeting each other in person for the first time at last week’s British Intrapartum Care Society Conference. And we won a prize! We are so grateful to the women who have participated in our research, the Principal Investigators who have made it all happen locally, and our Steering Committee. Here’s what we shared at the conference:
Dr Siddesh Shetty and Dr Shawn Walker
Is it feasible to test OptiBreech Care in a clinical trial?: results of the OptiBreech 1 study – Dr Shawn Walker, Tisha Dasgupta, Siân Davies, Sarah Hunter, Phoebe Roberts, Prof Jane Sandall, Prof Andrew Shennan. We shared the results from our first-stage study, OptiBreech 1. We are currently writing these up in publication format and will share as soon as that is ready. This presentation won the top oral abstract prize at the conference.
The roles and responsibilities of breech specialist midwives in the OptiBreech Care Trial feasibility study: a qualitative inventory – Davies, Dasgupta, Natasha Bale, Alexandra Birch, Walker. Siân Davies shared a poster about the role of Breech Specialist Midwives, as described by midwives and obstetricians participating in OptiBreech 1.
Toolkit for implementing breech clinics and specialist midwives to support planned vaginal breech births – OptiBreech PPI Lead and Service User Representative Phoebe Roberts presented this poster. Read more about it here.
Women seek ‘connected autonomy’ when they wish to plan a vaginal breech birth at term: a systematic review and meta-synthesis – Ritika Roy, Cecelia Gray, Charlene Prempeh, Walker. Medical students Roy and Gray presented the results of their 2021 King’s Undergraduate Research Fellowships. The results are ready for publication and will be shared in that format soon!
Not too fast not too slow: the legacy of time management in vaginal breech births – Jacana Bresson, Walker. Midwifery student Bresson presented the results of her review of obstetric texts in the Royal College of Obstetricians and Gynaecologists and Wellcome Trust Libraries, funded by a 2022 King’s Undergraduate Research Fellowship.
Assessing feasibility of economic evaluation alongside a full trial for ‘OptiBreech Care’ with development and testing of a decision model to assess its long-term cost-effectiveness – Dr Siddesh Shetty, Dr Shawn Walker, Prof Julia Fox-Rushby. The Health Economics team used this as an opportunity to gain feedback and peer review on the economic model developed.
Thanks also to the BICS Committee, who organise a wonderful, supportive, multi-disciplinary conference every time!
After last week’s #BICS22 conference, people have been asking me why @BICSoc is so special for me. This is what I tell them: (🧵of 7… all opinions my own)
Help us get it right, Wednesday 19th January 2022, 12:00-13:00. Are we accurately reflecting your views on breech specialist midwives and clinics?
We would like to invite women, birthing people and their families who have experienced a breech pregnancy at term to attend an online focus group discussion on Wednesday 19th January 2022, 12:00-13:00 to be conducted via Microsoft Teams. Anyone with an interest and experience of breech pregnancy can participate.
The purpose of this meeting will be to get your perspective on the work we have been doing so far.
We have been working on analysing data from qualitative interviews held with OptiBreech 1 participants. To date, we have interviewed 15 women purposefully sampled to reflect various OptiBreech sites, mode of births, and outcomes. Our main objective was to understand what makes the OptiBreech intervention acceptable (or not) to women.
The key themes that we have found are:
Access to skilled breech care: Vaginal breech birth as a viable and safe option is still unknown to many, and lack of specialists reduced equity of access. Women who were referred to a specialist at one of the OptiBreech sites or were already receiving care at a study site found it easy to access and participate in their care. Women who had to transfer care from another hospital or find an OptiBreech site themselves had a difficult time doing so, often requiring increased effort, multiple trips, time off work etc.
Balanced information: Women really appreciated being provided balanced information on the safety and risks of vaginal breech birth vs. caesarean section including possible complications and how to manage them. This enabled them to make autonomous informed decisions and increased self-efficacy and confidence, not only in themselves but also in the breech specialist midwife. Conversely, when women had to do this research themselves because they were not getting cohesive information from the healthcare professionals, this was seen as a burden and sometimes women were made to feel pressure to choose caesarean section as the ‘safe’ choice.
Shared responsibility: Women often felt emotional burden including feelings of stress, judgement, and guilt because of the choices they had made to have a vaginal breech birth, both from family and friends, as well as other healthcare professionals. Speaking with and being cared for by the OptiBreech specialist midwife helped ease this emotional burden and gave the women confidence in their choices.
Team dynamics: We found that women had placed an enormous amount of trust and confidence in the breech specialist midwife which extended to the rest of the team, attributed to previous experience, skills and knowledge. Although women did not know all the members of the team, the trust and confidence was extended to them because of shared responsibility and training requirements needed by all OptiBreech team members.
We need your input on our findings and invite your opinions on whether these findings are relevant to you, if we have interpreted them correctly, or if we have missed any important factors in what makes OptiBreech an acceptable intervention. At the meeting we will present a short summary of our findings so far, and then have an open discussion to hear any thoughts, opinions, or questions you may have.
The meeting will be held on Wednesday 19th January 2022, 12:00-13:00 via Microsoft Teams.
Round 1 of the international multi-stakeholder Delphi study, Development of a Core Outcome Set for Effectiveness Studies of Breech Birth at Term (Breech-COS) is now open. We invite the involvement of anyone from the following stakeholder groups, who has experience of care for women having vaginal breech births:
QR code for Breech-COS Round 1
obstetrician
midwife
service users (you or your partner have had a breech-presenting baby within the last 5 years)
neonatologist
researcher
health services manager
healthcare commissioner
health economist
statistician
support group representative
other relevant roles
You can read more information about the research and participate using the link or the QR code below. You are welcome to share this post or forward to your stakeholder associates.
We are in the process of developing the protocol and study materials for Stage 2 of the OptiBreech study which will be a multi-centre prospective observational cohort study designed to support multiple trials of care for women with a breech pregnancy at term.
In the next phase of our study, we will begin to record outcomes for breech pregnancies and births from several more hospitals across England, Wales and Scotland, on a large database. Personal information, such as names and NHS numbers, will be kept separately from information on the outcomes of pregnancies, so that those who participate are not identified by anyone looking at the data. We will need to collect a lot of data and store it for a long time, so it’s important we get this right. We want to ensure we are providing information about the study in a way that is clear and ethical.
OptiBreech 2 will involve randomly allocating women to different care pathways, and creating a large scale database of term breech pregnancies for the purposes of 1) establishing safety outcomes in real-world settings and 2) conducting multiple nested trials to establish effectiveness of interventions in the breech care pathway.
Also, we will be asking some women to allow us to assign them by chance to one treatment or another; this is called ‘randomisation.’ Assigning people by chance enables us to be sure that any differences we see in outcomes are due to the treatment and not something else. For this reason, evidence obtained following random assignment is considered the highest quality evidence. We would like to know how you feel about this and how we are proposing to do it.
We would like to hear your views on the acceptability of randomisation as well as on the Participant information sheet and Consent forms (linked below).
We’ve created a Participant Information Sheet, with information about the study, and a Consent form, which we would need each participant to sign. We would like to ensure these are clear. And we invite you to tell us if you think we should be doing something differently.
The meeting will be held on Wednesday 16th June, 11:00–12:00 via Microsoft Teams.
You are invited to an open discussion about the Draft of the new NICE Antenatal Care Guideline. Breech Birth Network would like to collect the views of families who have experienced a breech presentation at term and care providers on the draft guidance. Josephine and Thiago talk about their experience of Ulysse’s breech birth at…
We invite participation in an on-line PPI (patient and public involvement) meeting to be held on the 10th of December.
We would like to invite women, birthing people and their families who have experienced a breech pregnancy at term to attend an online focus group discussion on Thursday 10th December 10.30-11.30am to be conducted via Microsoft Teams. Anyone with an interest and experience of breech pregnancy can participate.
The purpose of this meeting will be to get your perspective on the following issues:
A core outcome set is a minimum set of outcomes that should be collected in every study about a topic, in this case vaginal breech birth at term. Making these consistent means that we can better compare and combine studies, and ensure research meets the needs of those who use it.
To develop a core outcomes set, we have conducted a systematic review of the available literature relevant to this project (brief summary below). However, we need your input to determine if these outcomes are important to the people who will use the results of research to make decisions, and how important each is. Does this meet all your informational needs or are there outcomes that have not been identified, which you think is important to record?
Do you think it is important to include salutogenically focused outcomes that emphasize positive well-being of the mother and newborn such as maternal satisfaction, relationship with baby etc.? If so, which factors would you like to see and how important do you think these are?
The next stage will be to ask both professionals and service users to rate the importance of the outcomes to be included in the core outcome set. But before we do this, we want to insure all of the outcomes important to you are included.
You are welcome to share your feedback directly during the focus group meeting or by emailing Tisha Dasgupta (tisha.dasgupta@kcl.ac.uk), the OptiBreech Research Assistant, at any point. If you are unable to make it and would like to contribute, or have further feedback after the session, please also contact Tisha.
While we do not require written consent for your participation in the meeting, it is important to let you know that the session will be recorded. We intend to take the feedback you provide into consideration while designing the next stage of this project: a multinational Delphi study. No identifiable information will be used such as direct quotes or anecdotes, and we will only report summary data.
Thank you very much for your consideration. Please could you send your RSVP to tisha.dasgupta@kcl.ac.uk by Monday, 7th December to confirm your attendance at the session? She will be in touch thereafter to provide you access to the online meeting.
We’d also love to hear your views on the information presented on the OptiBreech website!
Overall summary of the Systematic Review
A systematic review of all relevant literature was conducted to identify outcomes, definitions and measurements previously reported in effectiveness studies of breech births at term. 108 studies were identified comprising of systematic reviews, randomised controlled trials and comparative observational studies, with full-text available in English. Below are the most common outcome measures, with a percentage of how many studies reported them. These are the top 10 most frequently reported measures in each category grouped by neonatal, maternal, features of labour, and long-term maternal outcomes respectively.
Neonatal outcomes
Outcome measure
% studies reported
APGAR score at 5 minutes
78.7
Perinatal or neonatal mortality
68.5
Admission to neonatal intensive care unit (NICU)
59.3
Neonatal birth trauma/morbidity
53.7
Brachial plexus injury / peripheral nerve injury
38.0
Low umbilical artery pH
35.2
Bone fracture
33.3
Neonatal seizures/convulsions
31.5
Intubation/ventilation
29.6
Hematoma (cephalic or subdural)
20.4
Maternal outcomes
Maternal mortality
24.1
Post-partum haemorrhage (PPH)
16.7
PPH requiring blood transfusion
14.8
Other serious maternal morbidity/other complications
Each time I teach the Breech Birth Network Physiological Breech Birth Study Day, I explain the feasibility study and trial I am hoping to do and invite feedback from those attending. Below are examples of feedback from around the UK:
Hayward’s Heath, December 2019 — Princess Royal Hospital
Some surprising feedback in a recent meeting with the Lead Obstetrician and Director of Midwifery in one of the South London teaching hospitals who are not currently planning to participate in the randomisation element of the feasibility study. This hospital is further along implementing a breech clinic and some on-call element to support physiological breech births. Because of this, they feel it might be unethical to randomise women to ‘standard care,’ as outlined in the Description of Intervention. They will still be participating in the implementation evaluation aspect of the feasibility study. I and the Steering Group will be considering this and feedback from other Trusts when deciding if the final design should be modified in a larger study.
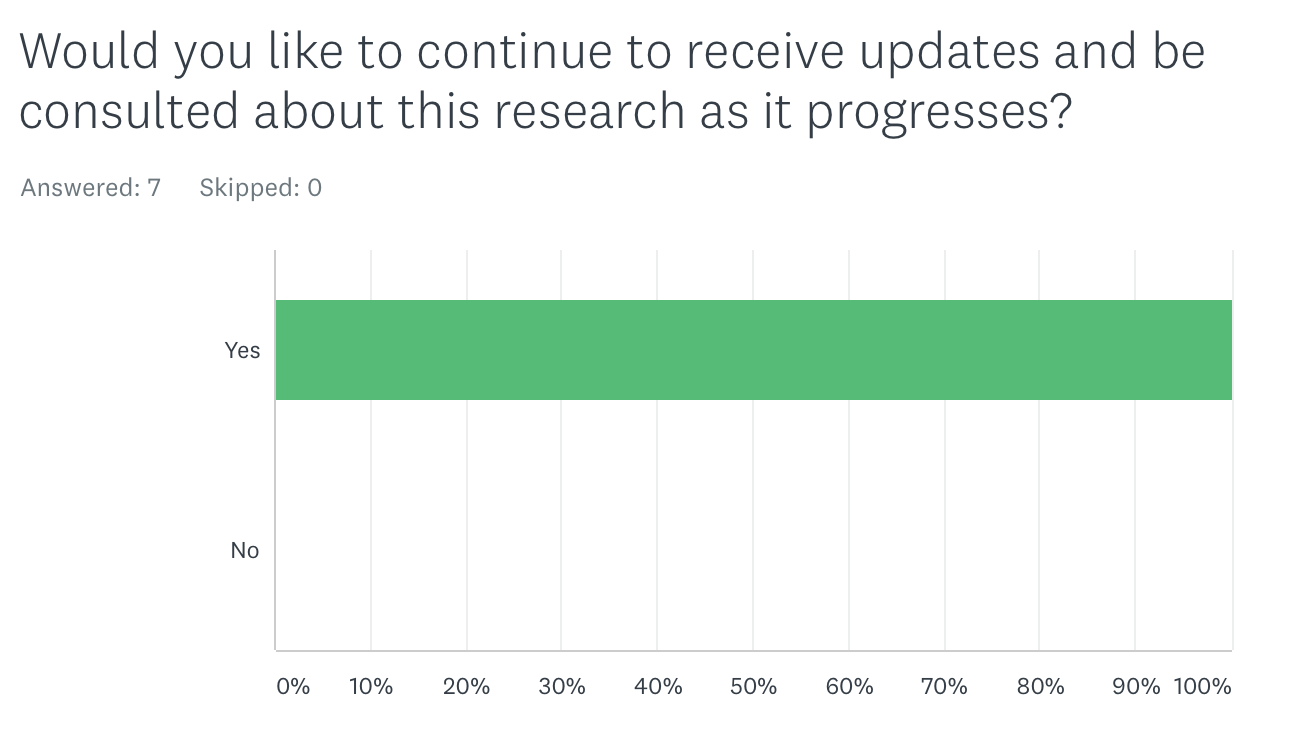
In addition to face-to-face activities, when developing this proposal I circulated an invitation to participate in PPI via my professional blog (breechbirth.org.uk) and social media. Twenty-one women and three people who work with pregnant women (midwife, doula, osteopath) expressed an interest. Some of these women attended the face-to-face meeting at St Thomas’ Hospital in April 2019, organised by the South London Maternity Voices Partnership. I met with two women individually in East Anglia, and seven women responded to a survey (via SurveyMonkey) asking about their views on the plain English summary of my proposal. This post reports the responses of these seven women to this summary and how this has influenced the form of the final proposal.
All comments are reported and all women were asked for permission to share these responses anonymously.
All seven women (100%) indicated that, “I or my partner have had a breech baby within the last 5 years,” within the UK. Comments included:
I had an undiagnosed breech vaginal delivery in 2015, in spite of having had numerous palpations/sweeps in the weeks leading up to the birth.
I experienced my own undiagnosed breech birth (vaginal delivery) in December 2015. Happy to provide in depth detail of my birth story; it is also published in my own work on this.
My breech baby was undiagnosed as breech, so I have no experience of what it feels like to contemplate the choice between natural breech birth or cesaerean. I am however part of various breech networks on social media and take part in many discussions about this. I had my breech baby at home, and unassisted, with no complications.
“I gave birth at home to my frank breech baby. I wasn’t supported by most of the health professionals I met and when it came to the birth it didn’t feel safe to go to our hospital where they were very short staffed and my labour progressed too quickly for me to get there! I trusted my body knew what to do and our baby was born safely with my just my husband watching! Paramedics arrived and our doula as our baby was born. The midwifes weren’t available for another 4 hours! It was a huge shame as they missed the opportunity to experience my calm, pain free, extremely well researched breech birth.”
Impact on proposal: ‘Undiagnosed breech birth’ means the breech presentation is diagnosed for the first time when the woman is in active labour, rather than during her antenatal care. Occurrences of undiagnosed breech births seem a significant component of ‘breech experience’ among women in the UK. My original proposal focused solely on management of breech presentations that are diagnosed antenatally, but I realised this is not enough. Also, the last randomised controlled trial of term breech births (Hannah et al 2000) included breech presentations diagnosed for the first time in labour. Although recruitment during labour is particularly challenging, PPI feedback indicates meeting this challenge is important.
These results were similar to those received in the face-to-face and staff PPI activities.
I think women will want to take part to ensure that breech pregnancies and births are better dealt with. Natural births of breech babies should be supported more, so this study will help.
I feel women would participate especially if they have had choice taken away from them. Enabling informed choice and joint decision making is crucial for all woman no matter what presentation.
Yes but only if they are reassured prior to birth that they will not be forced into a certain birthing choice because they signed up for the trial. I think constant reminders would be helpful to them that they still have choice throughout otherwise this could be a potential barrier to recruitment.
I felt very pressured during my pregnancy by doctors, and really struggled to make choices. (Whether to homebirth or not). I feel that any woman in this situation or who has had previous experience of hospital would be very glad to take part in something that could change the way women are treated and spoken to in hospitals. I personally would be willing to take part in any research that improved the way pregnant women are treated.
If the question is meaning the breech births that have already happened then it is likely the women will want to take part to help other women. If it is for women about to give birth to breech babies then it depends on how confident, trusting and educated her team of midwives and consultants are of breech vaginal delivery.
Influence on research design: At least some women find decision-making around mode of childbirth with a breech baby difficult, and that at least some women have felt pressured and have experienced a lack of respectful care. Ensuring this research does not result in harm of this type is important to me. This influenced the design in the direction of a pragmatic RCT. In the original proposal, I had planned to conduct an efficacy study, which requires strict adherence to group allocation. However, through engagement with women I came to feel this would not be ethical, nor would it provide the type of ‘real world’ decision-making information women wanted. Recruitment would also have been more difficult.
It will give women a better understanding of their options and what they consist of. It will help women come to the right decision that best suits them.
Empowering women to trust in their body’s natural ability will always be a positive thing
Yes, any additional information to what is already known will always serve to be helpful to women and allow them to make more informed choices.
I think there is very little information available on breech birth, and the stuff that is isn’t “readily” available unless you go looking for it and do your own research. I think newer studies and studies with more data are definitely needed and would provide women with up to date research and the information they need to make informed decisions.
Any extra research would definitely be helpful, the way the world is now it seems most people like statistics and there’s so much health and safety surrounding breech births in many hospitals/countries. Women are then too nervous by the lack of skill so they opt for a c-section.
This is fantastic! I gave birth to my breech baby in November 2017! It was the most incredible experience of my life where I truly tuned into my body. I did huge amounts of research during pregnancy and continue to do so now. Birth is incredible but breech birth is fascinating and it’s become my passion. I would love to be involved with this as much as possible!
Influence: I have created a mailing list to keep all respondents informed of the progress of this research and aware of any opportunities to contribute further, with clear information about how to remove themselves from the list and have any personal data deleted.
Below are some additional comments from women who did not participate in the survey, but expressed interest in PPI participation in general. Although I have anonymised responses, aside from one link the person wanted to share, they came from all over the UK. Women seeking support for a current pregnancy were referred to an independent breech midwife not involved with this research, with their permission.
I just came across this. I’m don’t work in the medical profession but my baby was a breech baby. I requested a vaginal delivery which was very negatively received by my hospital. I very much wanted to attempt it, which I did (in the understanding that if it became too dangerous I would agree to a c-section) However I have found out from a report that the second stage of my delivery was very poorly managed and sadly my baby died just after he was born. I was very much made to feel Like it was my fault for the birth choice I made. I truly wish there had been more open discussion about how my hospital felt about it and why they were so reluctant to support me. Breech birth should be talked about and openly discussed more. Great that it’s finally happening.
I experienced primi breech vaginal birth under Dr X in X Hospital, X city in 2014. I had a doula and I’ve trained to be a doula since. Breech birth in hospital can and should happen, and happen safely. I’m interested in being involved if I can be of use.
During my last pregnancy we found out baby was footling breech at about 36 weeks during a growth scan. Previous to this all midwives and doctors has told me he was head down. I had an ecv and went on to have a successful vaginal birth at 41 +3
I had a breech baby by (reluctant) c-section 3 years ago. There was a general lack of experience in vaginal breech birth in my area.
My daughter (born November 2016) was undiagnosed breech. My waters broke and instead of waiting for the normal 24hrs, the obstetrician recommended an induction as the midwife had picked up a small drop in her heart rate. It was the obstetrician’s opinion that the drop was probably due to position but still no one noticed she was breech. The diagnosis came when I was 5cm dilated and a midwife felt the my daughter’s bum during a VE. I wasn’t given much of an option then and whisked into an emergency c-section.
I’m pregnant again and though still early (28 weeks) baby is currently breech too. I’m trying to explore all my options and to be prepared for different scenarios this time round, but am finding that a lot of the research I come across is inconclusive. If there’s anything I can do to help, I’d be very happy to contribute.
Im currently pregnant with extended breech baby. my second pregnancy. no risks.
I would like to consider the natural birth. Doctors recommend CS but I don’t feel I got all the information to make informed decision.
I heard confusing message like we have no experience which is concerning and no statistics but more list of things which can go wrong.
I would like to find out pros and cons so I can make informed choice.
I would appreciate if you can get in touch with me.
I am 38.5 weeks pregnant.
I’ve stumbled on your website by chance. I had a breech baby in October 2016 at X Hospital. We didn’t discover breech until 41 weeks and at that point I was immediately coerced into agreeing to a c-section which was performed less than 12 hours later. I found the experience highly traumatic and ended up with anxious episodes (flashbacks/obsessive thoughts/nightmares etc etc) which required counselling.
I would love to be able to help with your research in the hope that future women do not have to experience what I did.
I’d like to register my interest. I had a breech pregnancy in 2014 which resulted in a Caesarean section.
I’d love to help in anyway possible. I’m currently a final year Midwifery Student with a passion for VBB and the topic is also my dissertation topic.
Definitely interested in helping in any way with the research!
I used this site and many others in order to make a decision about my recent birth. My baby was extended breech for most of the pregnancy and after reading as much as I possibly could about why a possible vaginal delivery was possible I declined the elective section and waited for natural labour to happen.
Supported by my NHS midwives, I went into labour and made the plan to labour naturally in hospital for a set amount of time and opt for no intervention and an emergency c if things didn’t progress. After an amazing 22 hour labour, a few hours fully dilated with faint declining contractions and no desire to push and no descending baby, I opted for (a calm and requested by myself) “emergency” c and was so happy to have been given the opportunity to give natural birth a good go, and know when to call it a day and not force it.
I wanted to share my story but am really happy to be involved in any research. I was only able to make a decision about my birth as I asked CONSTANT questions and read every single possible thing I could about breech birth. More information definitely needed so women can also make this decision for themselves and like me, EVEN thought I had an emergency c, come out the other end ELATED with their experience as they know they made all the right decisions based on information and not scare stories or sweeping statements.
Thanks for listening 🙂
I am currently 40 weeks pregnant with a breech baby hoping for a natural delivery and I would like to be involved in this project.
I had a very happy breech birth experience in February this year at X Hospital in Wales, X. I was due to have a c-section but went into labour early and then opted for vaginal birth, with encouragement from team of medical staff. Incredible midwives guided me through whole process. I feel so pleased and privileged to have such a positive birth story.
I had an undiagnosed breech vaginal birth 15th March 2015. My daughter had no complications and neither did I. She was born at 40+1. I would be happy to take part in any studies that I may be able to help with.
I saw on the X Facebook page that you are conducting studies on Breech babies.
Unfortunately I’m not available on 29th April but would be happy to help in any other way I can.
My daughter now 13months was a breech baby and I desperately wanted a vaginal birth so had to ECVs to try and turn her. They were both unsuccessful. I refused a planned c-section hoping to deliver vaginally but after 18hours of labour which didn’t progress very well I eventually had a c-section out of fear of endangering her life.
I wish there had been more support to enable a vaginal delivery. I felt that most staff didn’t feel confident enough to support and allow a breech vaginal delivery.
In developing this proposal, I sought feedback from clinical leaders in the participating Trusts, as well as my research support team and personal international network of breech clinicians.
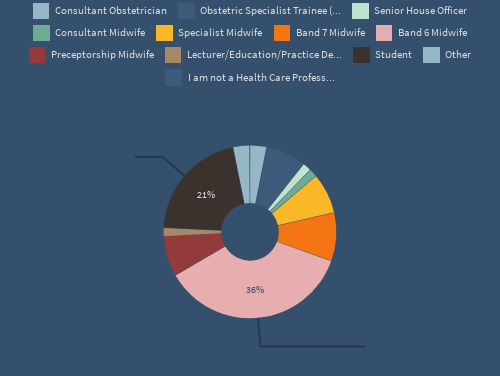
In May 2019, a Physiological Breech Birth study day was held at St Thomas’ Hospital in London. This included presentation of the feasibility study design, with an invitation to provide feedback via the Poll Everywhere app.
A total of 77 people attended the day. Information on their backgrounds is below.
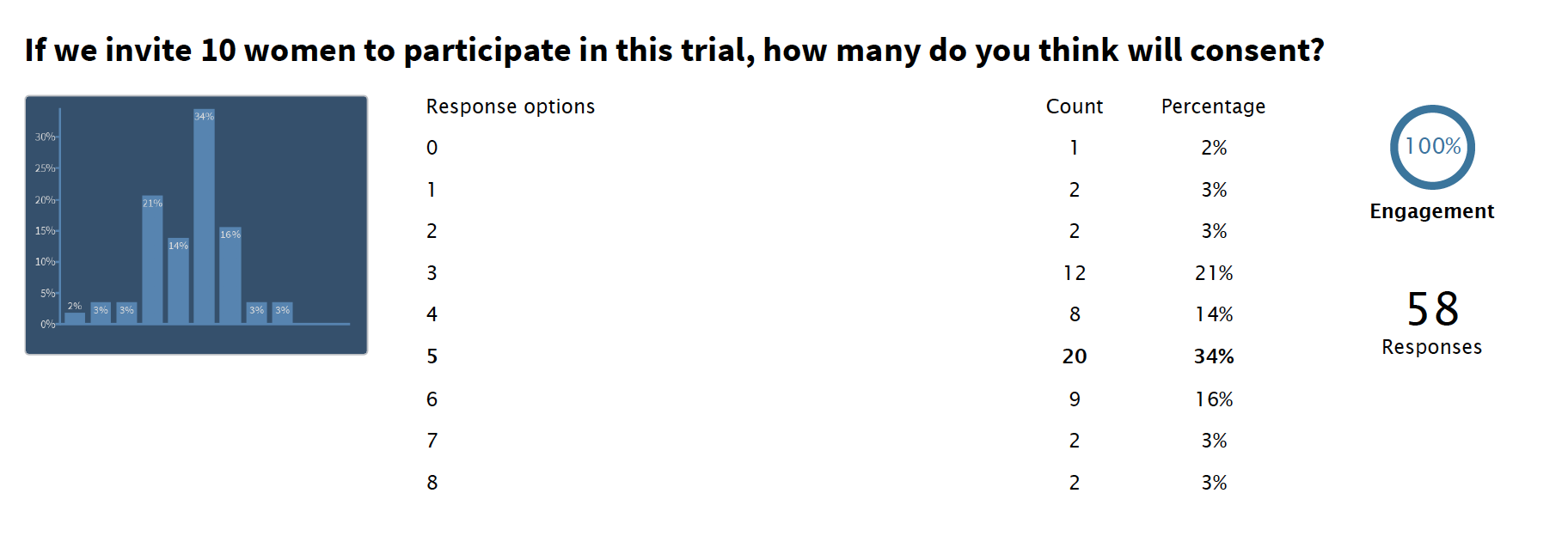
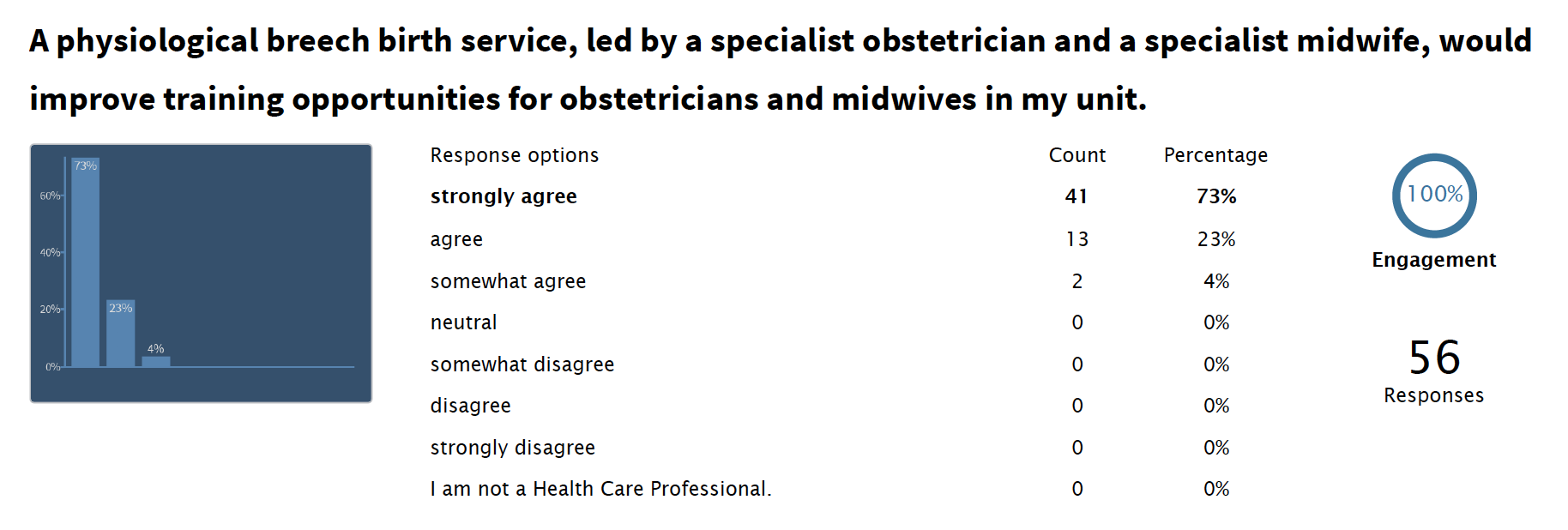
All attendees received a Description of Intervention and an explanation of the feasibility study design by the Chief Investigator. We asked health care professionals and trainees how many women they felt would be willing to participants. Their responses ranged from 0-8, with a mean of 4.3. This was slightly lower than predicted by PPI work with women.
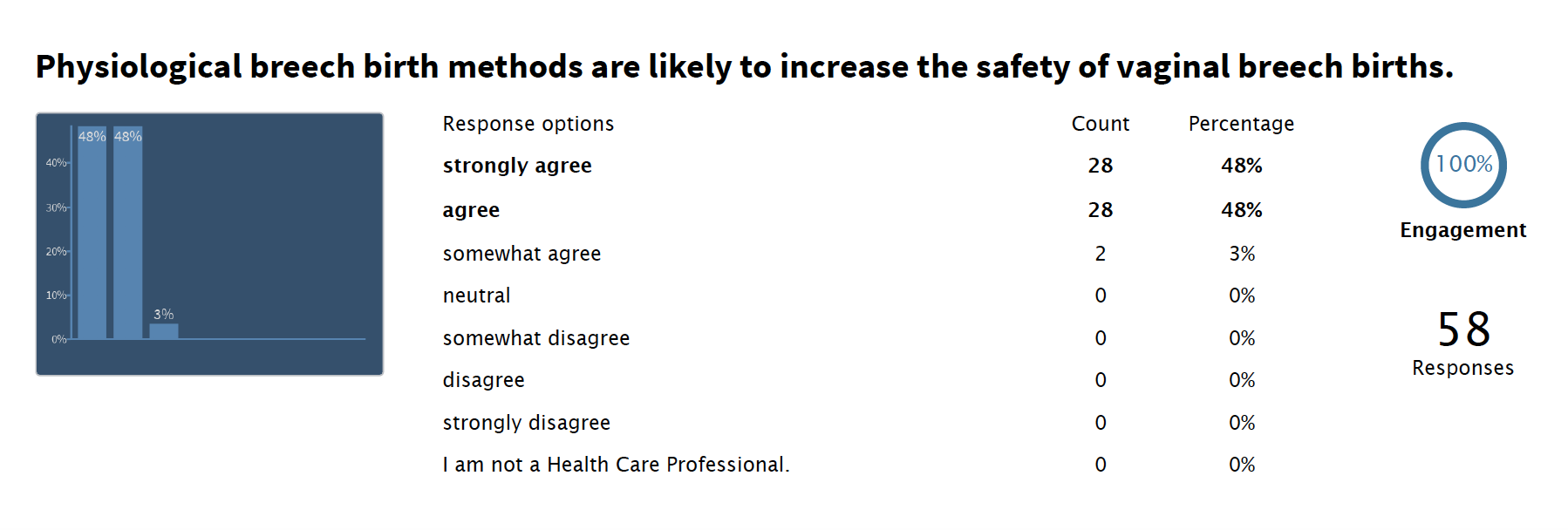
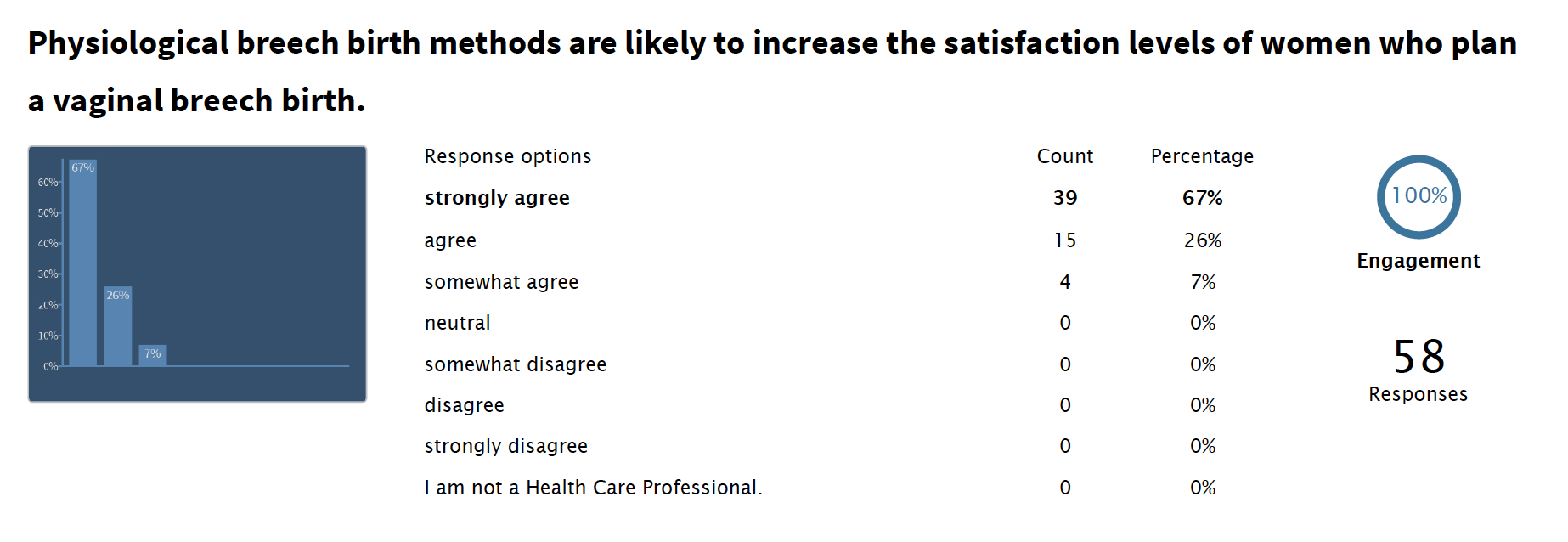
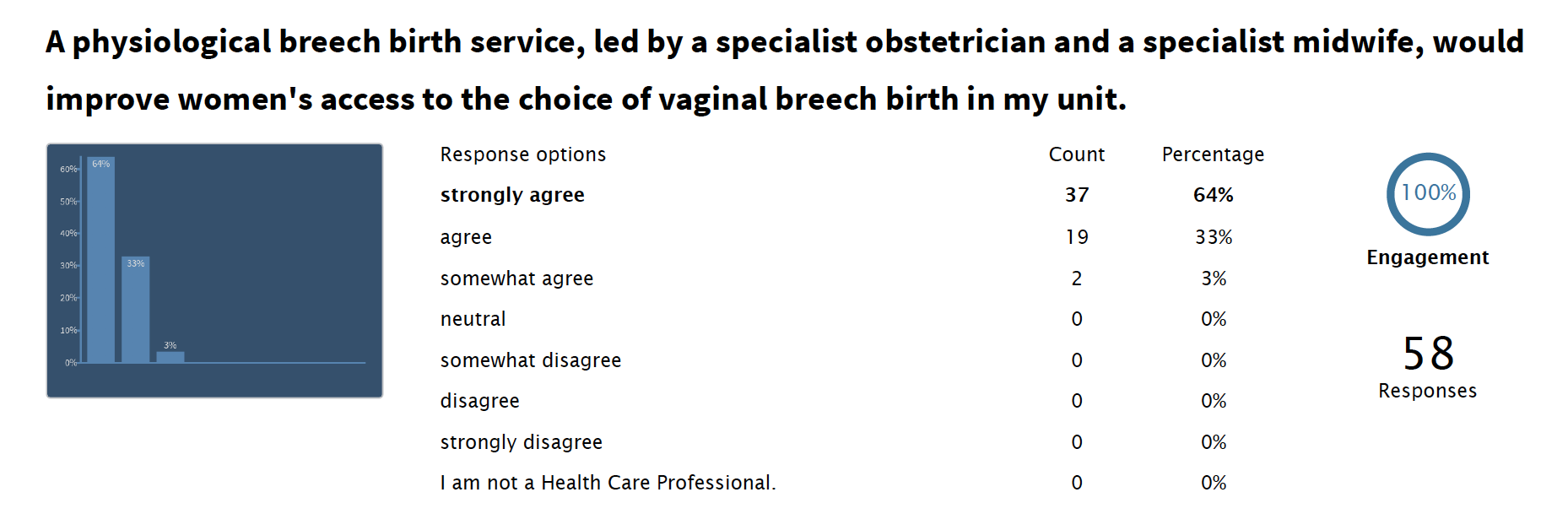
Reassuringly, after learning about physiological breech birth and the proposed feasibility study, professional opinions about the potential of the intervention appeared largely positive. But this was a self-selecting audience who chose to attend the study day and may not reflect the opinions of the wider maternity care team. And not everyone who attended the day was able to stay until the end to complete the survey.
Physiological Breech Birth care depends on a portion of health care professionals being willing to work flexibly in order to ensure experienced support at breech births. Feedback indicated that, although this was not something every practitioner was willing to do, a sufficient number to create a breech team was likely to be achievable.
Read more about health care professionals’ responses to the feasibility study design:
The importance of complete and understandable information about the feasibility trial and about the option of vaginal breech birth was echoed across feedback from all sources. This has been highlighted as the main ethical issue in the Detailed Research Plan.
As the protocol develops, I will engage carefully with those who have indicated an interest in remaining involved in the feasibility study to ensure information meets women’s needs. My colleague Emma Spillane, breech midwife at St George’s Hospital in London, has been developing an information leaflet about options for breech a term. This includes infographics, which women with autism and information processing challenges have fed back is very helpful. I will build on this for the feasibility study.
We will also look carefully at the number of women who are not able to participate in the trial because of informational barriers, such as the inability to understand written English. This will help to understand what translation services, into what languages, we may need to make use of in a full trial to enable equity of participation and access.
Lay reviewers from the RDS London Fast Track Service expressed concern about the legal situation should an adverse outcome occur with a vaginal breech birth. Women in both arms of the trial will be able to choose their preferred mode of birth. The difference is: women under physiological breech birth care will be offered assurance that, if they choose to plan a vaginal breech birth, the team will do everything possible to ensure they are attended by someone who is trained, skilled and experienced in physiological breech birth. In many NHS Trusts, the availability of such support is uncertain, as it depends on who is on shift in the labour ward on any given day/night. Women will be counselled as per the RCOG guideline and local guidelines regardless of their group allocation. They will be informed that we are doing this trial because the available evidence indicates that the physiological breech birth approach may improve access to and outcomes of vaginal breech births, but that we are not certain – hence the need for the research.
Will women participate in this research?
Designing a trial that would produce useful information for women, using methods that were acceptable to women participating in the research, was an important priority to me. The Term Breech Trial46experienced recruitment difficulties, which may have influenced the results.35 Early feedback moved the trial design in a more pragmatic direction, to a design that enables women to have the final say in whether they have an ECV and how they give birth to their breech baby. Another benefit of this design is that it will enable us to study how this new model of care influences women’s perception of the choices available to them.
When we asked those who attended the MVP meeting how many women out of 10 they thought would agree to participate, the range of answers was 5-8, with an average of 6.66. To increase enrolment, MVP members recommended a second recruitment opportunity immediately prior to any scheduled ECVs. This will give women time to think about it, and research midwives ability to identify potential candidates who may not have been offered the opportunity to participate immediately following their scan. This has been incorporated into the trial protocol.
One concern was that all women who participate would want specialist care, and would be disappointed if randomised to standard care. Although making specialist care unavailable outside of the trial is necessary for this design to succeed, and there was general agreement and understanding about this, some women felt it was unfair. For this reason, when a decision is made about whether to proceed to a full trial, we will consider whether randomisation at the individual level has worked. We will compare this to feedback from Trusts who indicate a willingness to participate in a full trial. Following the completion of the feasibility study, we will consider whether the current design will work. If not, and if enough Trusts are keen to participate, another design may be more appropriate, such as a stepped wedge cluster randomised controlled trial. In this type of research, individual Trusts would be randomised to implement physiological breech birth care at different times, rather than individual women.
What about the women who have had negative experiences of breech birth? Or those who are happy with standard care?
Women who respond to a call for involvement in development of a breech birth trial are more likely to have had either positive experiences of breech birth or negative experiences finding a lack of experienced support, for either planned or unplanned breech births.
Thank you to Maureen Treadwell of the Birth Trauma Association for helping me ensure this proposal is informed by the experiences of women who have felt traumatised by not being able to plan a vaginal breech birth, as well as those who have felt traumatised after planning a breech birth that did not go to plan. Women who have had negative experiences of breech birth may be more reluctant to engage in discussions about a breech trial, for very good reasons. Service user advocates like Maureen, who listen carefully to the stories of many women across the UK, help these voices to be heard as we strive to Do No Harm.
Maureen and the BTA highlighted that the goal of any further breech research should be to increase the quality of information and the availability of choice for women carrying a breech baby at term, rather than as part of a strategy that to reduce the CS rate.
This resonated with feedback from the RDS London Fast Track Review Service, through which four public representatives provided a review of two versions of the Plain English Summary. Again, the views of the general public about breech birth research are likely to be different to those held by women who have experienced a term breech pregnancy themselves. One RDS reviewer expressed concern that if physiological breech birth were deemed ‘safe,’ women would feel pressured to choose a vaginal birth rather than a CS, and this would undermine the priority of ensuring women are well supported regardless of their choice of mode of birth.
Thank you
… to everyone who took the time to respond to my research proposal, to members of South London MVP for giving me permission to share their feedback and to Alison Bish for co-ordinating responses from RDS London. I am extremely grateful and confident the design is better for everyone’s involvement.
If you would like to view the tool I used for the Maternity Voices Partnership Meeting, you can download it here.