Avni Batish and Kate Stringer, photo by George Haroun
On May 8th, we will be holding an on-line meeting to establish a consensus on short-term outcomes in our Breech-COS study. We invite anyone with an interest to attend. Book here to attend.
A key element of OptiBreech Care is providing additional skilled and experienced staff at planned vaginal breech births (and unplanned ones too if we can manage it!) in line with the RCOG guidance.
We know this supports safety but traditionally it has been hard to achieve as the numbers of vaginal breech births may be few and far between, meaning limited experience and often limited or brief training. Most hospitals have < 1 hr a year for each of the common obstetric emergencies as part of their mandatory training, maybe less depending on each hospital’s rolling program of multidisciplinary skills and drills. Furthermore, expecting whoever is on and available to care for families having a Breech birth puts significant extra stress and strain on the on-call labour teams, often already pressured with complex scenarios and sadly short-staffed wards.
We often get asked- How to do the on-call elements of the OptiBreech care pathway work? Who will cover it? Everyone is doing enough already?!
Each of our current sites may operationalise its on-call systems slightly differently, however, the core elements are the same.
All sites need to create a Breech team- ideally, this consists of a mix of midwifery and obstetric staff willing to be on call for breech births. Ideally, each member will have had some prior experience of a breech birth (although this is not always possible). All members of the Breech team should have completed a recent OptiBreech study day, online or face to face and have had an opportunity to practice rotational manoeuvres via simulation before providing on call for births. We would expect team members to counsel women appropriately regarding experience and expertise as part of the initial personalised care planning.
We would advise that initially, the On-call Breech teams are smallish. You may start with one or two lead people who are first on call with a wider group of staff that want to gain experience and eventually join a full on-call system.
We have found that this is the most successful way to safely develop confidence and competence amongst the team whilst also building a sustainable service. Often when launching the team in a service that hasn’t previously been supporting vaginal breech births, it can take a while for any to come along. Too large a team means that it is hard for people to gain regular exposure and experience and in the long run it takes longer to develop expertise.
Structure and payment of on-calls
All sites have currently been opting for a voluntary on-call system. At my site, many of the team have other on-call commitments (as manager on call or perhaps homebirth on calls) so they try to combine the calls and to date, no one has minded being voluntary on call. If called into the birth, they are always added to the roster to ensure liability coverage and this has worked wonderfully for the intrapartum teams as they are always grateful to have an additional presence with expertise available to support the team!
We have found this system has been provided at no extra cost to the service and has increased staffing on shifts which would have otherwise been under the template. Two of our core Breech team midwives work full-time in Intrapartum services so they have been available often when needed just by the pure nature of their roles and shift patterns. Whilst it is difficult for clinical midwives to be on the call before a shift, both midwives work full time so are already working a significant number of shifts. If one of the families booked for a vaginal breech comes into labour, the labour ward team always work to release them to support with birth as required. Another of our team works as a specialist midwife Monday to Friday and again has often been available during her working hours to support Breech births when needed or if called out overnight is able to rearrange her day as needed.
You will require one lead practitioner who can coordinate the Breech team and ensure appropriate care and on call coverage. Usually this will be the midwife leading the Breech Clinic but it could be an alternative depending on your context. The lead practitioner will provide details of the on-call service and then arrange with the wider team any dates they can’t cover.
In some sites, Breech teams prefer for women to contact them directly when they are in labour and the on-call team alerts the rest of the service, in other teams, the families will contact the triage service as per usual and then the Breech team will be alerted. Your system will depend on how your team is developed and your current on call working practices.
When women are in labour, other team members are invited to attend for additional experience and support, again this is facilitated voluntarily but we have found no problem with people wanting to be involved.
What if we have no one available or we don’t make it in time?
Sites need to make a realistic effort to try and support this as we know it improves safety outcomes and it is the core process outcome for the Optibreech care package but also women are honestly and realistically counselled. If no one from the team is available ( we know last minute dramas can happen) the care would fall to the rostered labour ward team and if they have limited experience in vaginal breech birth, they would counsel them as per their practice, which would usually be to recommend a cesarean birth.
Results from the feasibility study showed that across all sites a Optibreech team member was present for 87.5% of planned vaginal Breech Births.
We have found vaginal breech births have risen from 2 in 2021 to 10 successful (18 planned) last year with no admissions to special care and we have around 1/2 women a month planning a vaginal Breech birth. As our numbers have increased, we have been able to support more midwives and doctors able to lead the care and meet the full OptiBreech proficiency criteria. We are now considering implementing a more traditional on-call system to cover the whole month.
** A key aspect of care is the OptiBreech team member is addition to the case midwife. This is a pivotal part of the safety mechanism. The OptiBreech team member supports situational awareness, liaison with the wider MDT and ensures prompt action is taken if concerns arise**
Other OptiBreech sites operate similar variations to the above model, partly depending on their Breech birth numbers, initial expertise in the team and also taking into consideration individual contexts and staffing models.
Key aspects required for a Successful Optibreech On-Call Team
Motivated individuals with a desire and flexibility to work this way
A lead clinician to coordinate care, on-call availability and liaison with families
A small group of staff initially to enable ongoing enhancement of competency- this group could be expanded as numbers and confidence grow.
Dr Shawn Walker explains why the combination of meconium and tachycardia, particularly in the first stage of labour, indicates increased risk in breech births. OptiBreech teams offer women a caesarean birth when these occur together.
Warning: Birth images
Please join the OptiBreech Collaborative fetal monitoring case review seminar on Wednesday, 22 February, 8.30-9.30 – via Zoom.
Permission given to share this post and video freely with anyone who may find it helpful, including women in your care or colleagues.
Transcript
Hello. My name is Shawn Walker. I’m a Consultant Midwife, the Clinical Lead and the Chief Investigator of the OptiBreech Trial.
In this video, I am going to speak directly to women who may be planning a vaginal breech birth under OptiBreech care, but the information is also to inform the healthcare professionals who may be caring for you.
Within the OptiBreech Trial, we have observed an increase in complications among births where either meconium-stained amniotic fluid or fetal tachycardia are observed during labour, and especially when they are both present. I’m going to explain each of these things in turn so that you understand exactly what we are looking for and why our OptiBreech teams will be giving you advice they give you if they occur during your birth.
Meconium
First, meconium. Meconium is the baby’s first poo. When it first comes out, it looks like thick black tar. In a textbook, ideal vaginal breech birth, where the baby has coped beautifully in labour, this black tar substance first emerges around the same time we begin to see the place it emerges from! At this point, your baby is being tightly hugged in the final few moments before they are born, and it basically gets squeezed out of them like a tube of toothpaste. We’re fond of calling it ‘toothpaste meconium.’ This is completely, 100% normal and will occur in every breech birth.
However, when babies pass meconium before they are born, that’s a bit less straightforward. The meconium mixes with the fluid around your baby, the amniotic fluid. Professionals call this, meconium-stained amniotic fluid. It’s a fairly common occurrence. We see meconium in about one out of seven pregnancies. Occasionally, babies pass meconium when they are still inside after 40 weeks of pregnancy, or past their expected date of birth. Their bowels are more mature and ready to get moving, so they do. Sometimes it doesn’t mean anything more than a bit of extra mess.
But sometimes, passing meconium during labour is a sign that baby is finding it a bit stressful. Again, most of the time, babies can handle a little bit of stress in labour, just like their mothers. But if meconium is identified early in labour, we have advised our OptiBreech teams to err on the side of caution and offer you a caesarean birth. This is because we have observed that when we see meconium early in labour, we observe additional complications later in labour more often. There still may be a long way to go, and most women tell us they would prefer to avoid a rushed, emergency caesarean birth late in labour. The earlier we do a caesarean if it looks like it may be necessary, the more calm and relaxed everyone can be, and the safer it is for you and your baby.
So we want to offer you the information that there is some increased risk of this happening if meconium is present early in labour. But of course, this decision is always up to you. You may want to ask your OptiBreech team for more information about other signs that your baby may or may not be coping well with labour before you make this decision.
Tachycardia
The other way that your team can tell if your baby is happy during labour is by evaluating the baby’s heartrate. If you have chosen to start your labour with intermittent monitoring, using a hand-held monitor, the presence of meconium in your baby’s fluid would be a reason to recommend continuous monitoring. Professionals often refer to the trace from continuous fetal heart rate monitoring as a CTG, which stands for cardiotocograph. There are a few things we look for in a CTG trace to tell if your baby is coping well. But one of the things we consider important in a breech birth is called the baseline.
The baseline of your baby’s heart rate is another way of saying the average heart rate. Normally, this ranges from about 120 bpm to 160 bpm in labour. Just like ours, your baby’s heart rate fluctuates in labour. When your baby moves, the heart rate on a CTG often goes up, or accelerates, just like yours would if you are climbing a flight of stairs. We consider this a really positive sign of your baby’s well-being.
But if your baby’s heart rate climbs up to over 160 bpm and stays in that range, rather than settling back down to where it was when we first listened in during your labour, that is another sign that your baby is finding things a bit stressful. We call an average heartrate over 160 bpm a fetal tachycardia. Tachycardia is always a sign that your baby is compensating for something. This is likely to be either an infection or hypoxia, which means oxygen deprivation. Your baby can’t breathe faster, so instead their heart beats faster to circulate the available oxygen. Again, most babies cope well with this for limited amounts of time. That’s what they are designed to do.
However, if your baby is experiencing more than thirty minutes of tachycardia that does not settle in the first stage of labour, the team will offer you a caesarean birth. If this is the only concern in your labour, for example the fluid around your baby is draining beautifully clear, and we see lots of accelerations on the CTG as well, your care providers may be comfortable with observing for a bit longer. This is especially likely if your labour appears to be progressing very quickly or if your baby is near to being born.
Meconium AND tachycardia
But when these occur together – tachycardia AND meconium in labour – your OptiBreech team will change from offering you a caesarean birth to advising one, especially if these occur in the first stage of labour. When BOTH tachycardia and meconium are present, they are both more likely to be associated with infection and inflammation.
Thanks Shawn to highlight the significance of fetal tachycardia and meconium stained amniotic fluid in early labour – I must complement that the recommendation for cesarean section applies to both breech and cephalic babies.
When meconium is present in labour, in most cases, it has no consequence for the baby. But in 5% or 1:20 cases where we observe meconium in labour, the baby inhales meconium during the birth process and shows signs of what we call meconium aspiration syndrome after the birth. Meconium aspiration is more likely if the baby becomes severely stressed due to low oxygen levels and tries to take a breath before they are born. They then inhale the meconium-stained fluid into their lungs. This can result in breathing problems and require admission to the neonatal intensive care unit. This is more likely if infection or inflammation processes are present. In about 1:5 cases of meconium aspiration, there can be long-term problems for the child associated with this, again more likely if infection and inflammation are present.
We also think this may be more likely in breech births because of the way these babies are born. In every breech birth, there will be a period just at the end when the baby’s cord is likely to be compressed. When deciding whether it is safe to start or continue pushing, your OptiBreech team will be evaluating how long this period is likely to be, and how well your baby is likely to cope with it. Again, most babies cope very well with this for a short period of time, especially if we keep their umbilical cord attached after birth. But if your baby is ALREADY compensating with a raised heart rate and THEN the birth is difficult at the end, your baby may be more likely to inhale meconium-stained fluid.
For many years, the primary strategy to reduce risk in vaginal breech births was to try to predict which babies would have problems based on ultrasound scans – this baby is a bit bigger than others, this baby has a foot tucked below his pelvis, etc. But unfortunately, this strategy is not very accurate. A lot of caesarean births are recommended when the babies are not at significantly different risk to other babies who do not have these characteristics before labour.
In OptiBreech care, our strategy is to respond to emergent risks in labour. This means we look out for signs during the course of labour itself that your baby may be one of the few who do not do well with a breech birth, and we give you this information as soon as possible. Prior to labour, we simply cannot predict which labours may be affected by meconium or tachycardia. The situation in which a baby inhales meconium during birth and has some long-term issues as a result only occurs in about 1:700 births; and that includes all births, not just breech.
Meconium is only present in about 1 in 7 births, so when we see this in the first stage of labour, we know that the risk is now about 1:100. We know that aspiration of the meconium will only occur in about 1:20 births where the meconium is present, but when tachycardia is also present, this risk is closer to about 1:5. If one or both of these appear close to the end of labour, it may not be as much of a risk because most of the meconium may be coming down and out rather than circulating in the amniotic fluid around the baby. Your team may judge that your labour is progressing quickly and the safest thing is still continue with a vaginal birth. But when both meconium and tachycardia appear in the first stage of labour, our clear recommendation is for the team to calmly take you down the corridor and assist you with a caesarean birth, with your consent, due to the 1:5 risk of meconium aspiration with potential long-term problems.
I hope this helps explain why we consider meconium and tachycardia signs of potential risk for your baby, especially when they occur together, and even more so when they are present early in labour. I want to reassure you, that most babies will be absolutely fine, even if meconium or tachycardia occur during labour. Most babies are very resilient, like their mothers.
But the premise of OptiBreech care is that we are always honest with you about any potential increased risks that we detect. And we ask our teams to always honour your wishes about what you want to do with that information. We feel confident to support more people to attempt a vaginal birth because together, the OptiBreech collaborative are developing new guidelines, based on what we see happening in our research, to help keep you and your baby as safe as possible.
In developing this proposal, I sought feedback from clinical leaders in the participating Trusts, as well as my research support team and personal international network of breech clinicians.
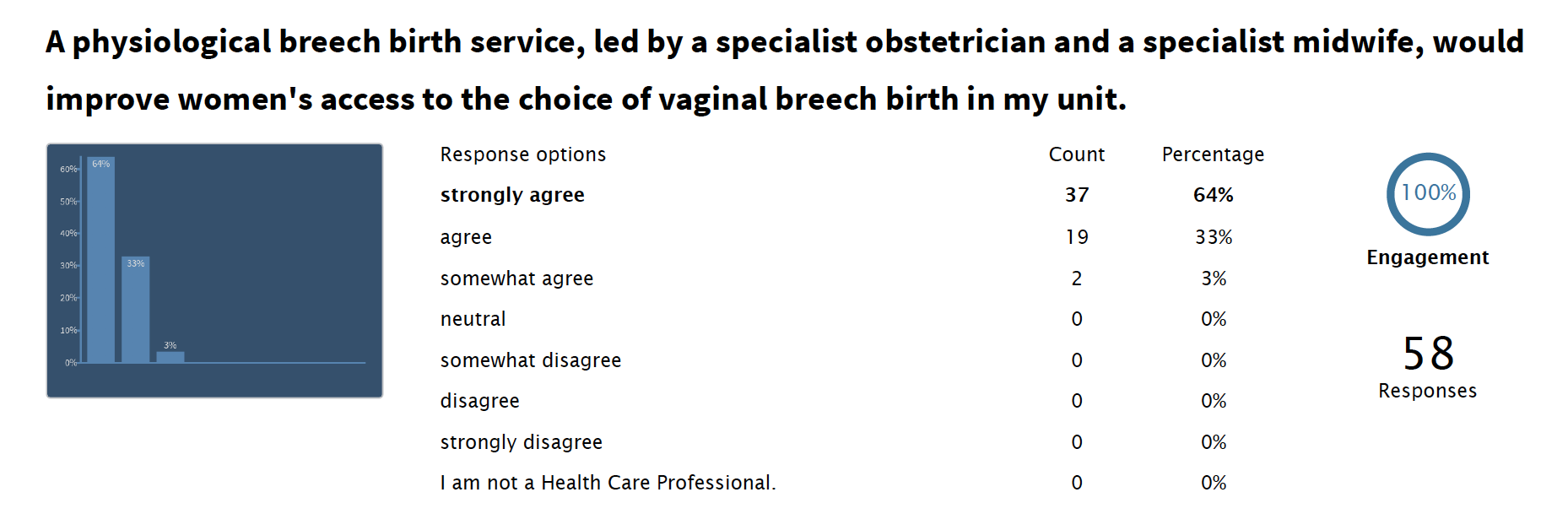
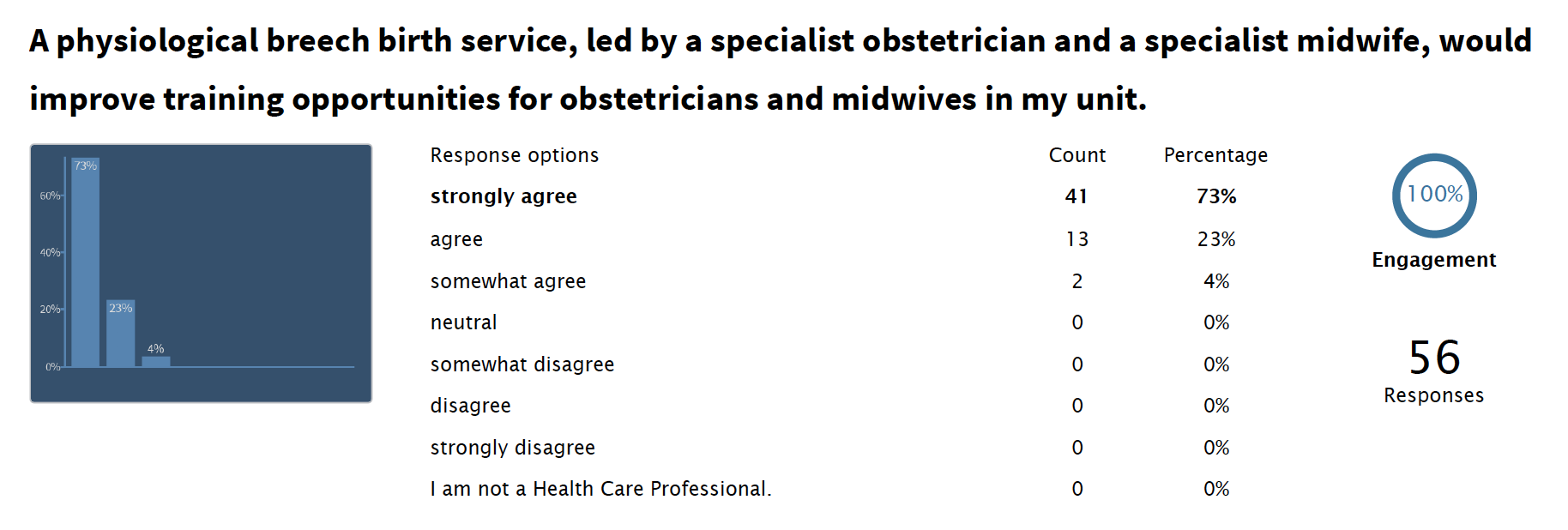
In May 2019, a Physiological Breech Birth study day was held at St Thomas’ Hospital in London. This included presentation of the feasibility study design, with an invitation to provide feedback via the Poll Everywhere app.
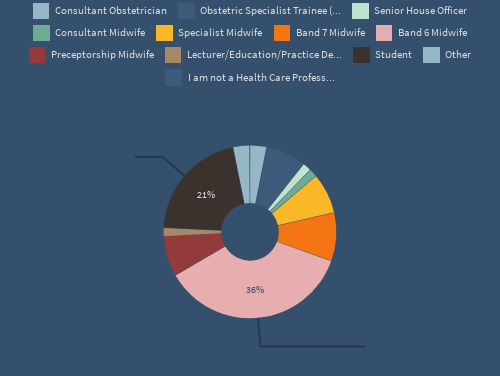
A total of 77 people attended the day. Information on their backgrounds is below.
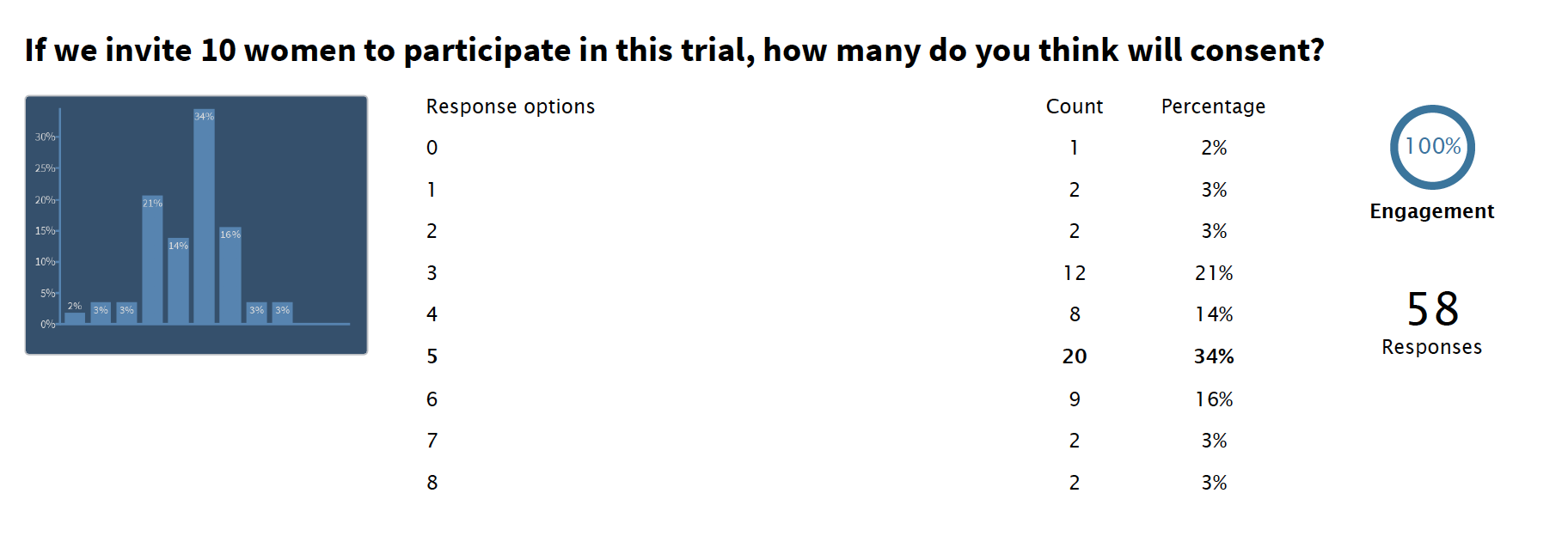
All attendees received a Description of Intervention and an explanation of the feasibility study design by the Chief Investigator. We asked health care professionals and trainees how many women they felt would be willing to participants. Their responses ranged from 0-8, with a mean of 4.3. This was slightly lower than predicted by PPI work with women.
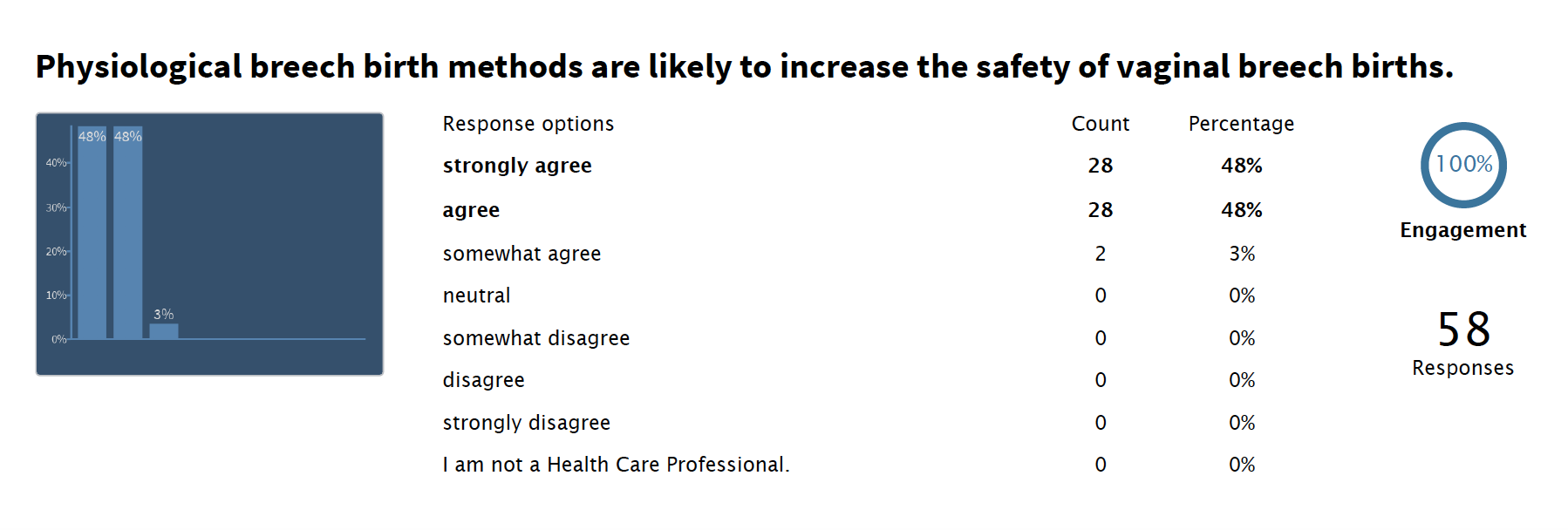
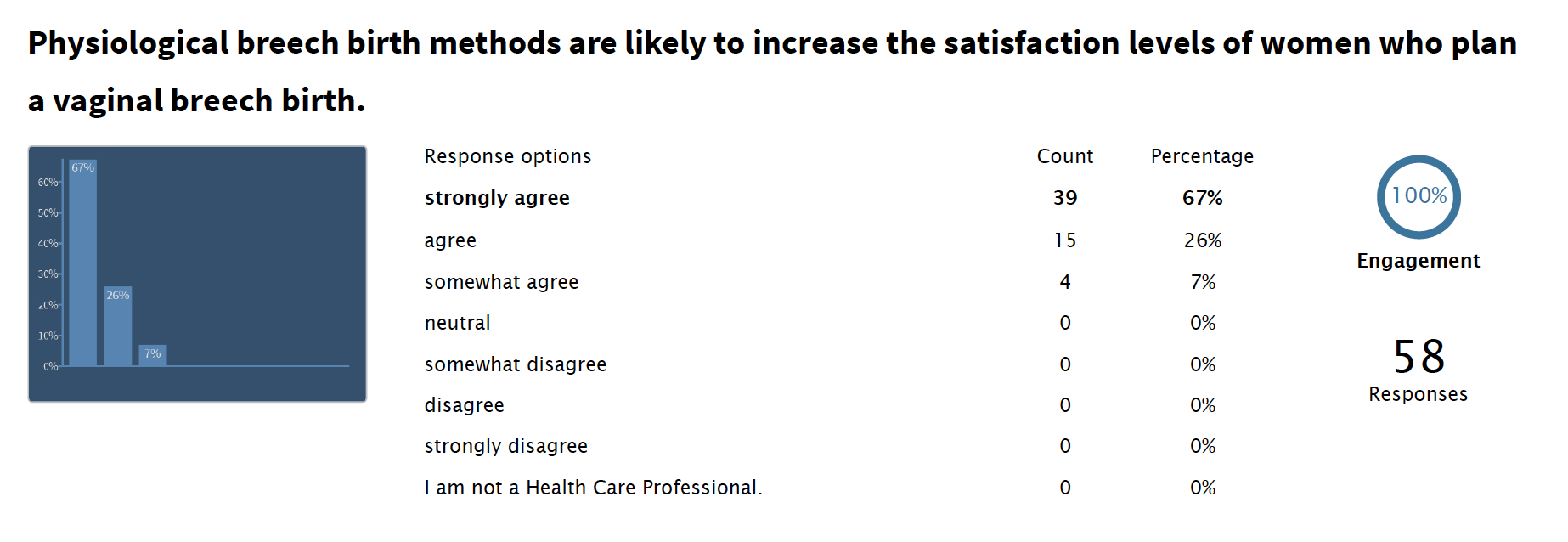
Reassuringly, after learning about physiological breech birth and the proposed feasibility study, professional opinions about the potential of the intervention appeared largely positive. But this was a self-selecting audience who chose to attend the study day and may not reflect the opinions of the wider maternity care team. And not everyone who attended the day was able to stay until the end to complete the survey.
Physiological Breech Birth care depends on a portion of health care professionals being willing to work flexibly in order to ensure experienced support at breech births. Feedback indicated that, although this was not something every practitioner was willing to do, a sufficient number to create a breech team was likely to be achievable.
Read more about health care professionals’ responses to the feasibility study design: