The second round of our consensus-building activity to establish a core outcome set for breech birth studies is now open. This will establish a standard set of outcomes and their definitions that ALL breech birth studies will collect, so that we can compare the results.
We have sent personal invitations to all previous participants but are also opening this round to new participants.
You can participate here. You are welcome to forward this post to anyone else who may be interested. The results will inform a consensus meeting discussion to take place in the spring. This will be open to the public and announced later this year.
We invite participants from the following stakeholder groups:
Service user (you or your partner has experienced a breech pregnancy)
midwife
obstetrician
neonatologist
paramedic
anaesthetist
health researchers
health service manager
healthcare commissioner
health economist
statistician
support group representative
Example of results from the first round on the outcomes of intrauterine death/stillbirth and cord clamping < 1 minute after birth.
The @OptiBreech team are looking to collaborate with service users who can help us share results with your communities
We have talked about the importance of inclusive research and ensuring the design of studies and trials are shaped by all voices recently. It is also important to consider the dissemination of results and ensuring we reach as many different groups as possible.
Currently, for 39% of OptiBreech participants, English is not their first language. We have a significant number of participants reporting Arabic, Polish, Portuguese, Romanian, Somali, Spanish, Tamil, and Urdu as their first language, with 13% of our participants indicating they need a translator. Additionally, 10% of OptiBreech participants are aged 25 and under.
We therefore would like to reach out to members of our involvement group and previous participants, to form an OptiBreech Results Group. We want to collaborate on developing a strategy to reach as many under-represented communities as we can who may not access our news and events through website updates or traditional media.
This may include making short, self-shot videos helping to communicate the results of our research in your own words and language, especially those results that YOU feel your community will find important. We welcome your ideas on how best to identify the most appropriate outlets to reach as many demographics as we can. You will be reimbursed for any activities with a Love2Shop voucher, in line with the NIHR’s recommended payment rates (approximately £25/hour).
We believe it is important to share data and evidence so that members of the public are aware of their options. We want everyone to have the information to be able to advocate for improved care for themselves individually or alongside their local Maternity Voices Partnership organisation.
Siân Davies, Participant & Public Involvement and Engagement (PPIE) lead.
To express an interest in helping us to disseminate the results of our research with your local community, please complete this form:
In recent years we have seen the pervasive effects of health inequalities and inequities highlighted in the MBRRACE-UK reports. There has been discussion since then about ‘hard to reach groups’ and how we ensure all voices are shaping research and clinical practice. However, Dr Natalie Darko, an Associate Professor of Health Inequalities offers the perspective that actually it is more a case of research being incredibly difficult to access for a number of communities rather than those groups being hard to reach.
This is an incredibly pertinent consideration and something research teams really need reflect on when in the initial stages of designing research. We have seen a real emphasis on co-production and PPI informing projects but to truly address health disparities, it is critical to ensure underrepresented groups are included and their voices are shaping future work.
I recently met up with Victoria Walsh, chair of Wirral Maternity Voices Partnershipto discuss some of the OptiBreech Project’s upcoming work and develop an inclusive PPIE strategy. We reflected on how best to be able to engage with a number of communities who are often excluded to increase their participation. Considerations such as interpreters (in multiple languages and British Sign Language) for events (both online and in person) and translation of all participant-facing materials to address language barriers. Accessibility should be considered in terms of the physical, psychological, technological, and financial barriers to participation. Additionally, mistrust in services is often a key barrier for underrepresented groups being excluded from research and so therefore consideration of our position and power must also be central to our approach when engaging with these communities.
We are proud that in our pilot trial, 59% of participants came from non-British backgrounds and 29% were from black or brown populations. But we know there is always more to do to ensure everyone can participate in research. We look forward to continuing to work with Wirral MVP during the course of this year to be able to remove even more barriers to maintain the diversity of participation in OptiBreech research.
Siân Davies – OptiBreech Research Assistant and PPI Lead
A photograph of my not so little breech baby!
Useful References
Coe D, Bigirumurame T, Burgess M et al. Enablers and barriers to engaging under-served groups in research: Survey of the United Kingdom research professional’s views [version 1; peer review: awaiting peer review]. NIHR Open Res 2023, 3:37 (https://doi.org/10.3310/nihropenres.13434.1)
Investing in staff and their skill development will achieve the same, if not better, results and should be the priority.
This a response to a recently published report in PLOS Medicine suggesting that implementation of universal third trimester ultrasound scanning in pregnancy improves outcomes for babies and mothers.
The following contributors have approved this expression of concern:
Researchers and Clinicians:
Shawn Walker, Researcher in Residence and Honorary Consultant Midwife, Imperial College Healthcare NHS Trust
Emma Spillane, Deputy Director of Midwifery and OptiBreech Lead, Kingston Hospital NHS Trust, London
Sabrina Das, Consultant Obstetrician and OptiBreech Lead, Imperial College Healthcare NHS Trust
Philippa Corson, Consultant Obstetrician and Breech Clinic Lead, Royal London Hospital, Barts Health NHS Trust
Susan Bewley, Emeritus Professor of Obstetrics & Women’s Health, King’s College London
OptiBreech Patient and Public Involvement Leads:
UK researchers have an ethical obligation to involve service user groups in design and interpretation of research studies
Siân Davies
Nimisha Johnstone
Norfolk and Norwich University Hospital Maternity Voices Partnership Service User Representatives:
Lisa Brophy
Marion Frey-Alqurashi
Rachel Graveling
Siobhan Ridley
Evelyn Shadlock
Knights et al1 confidently demonstrate that routine third trimester, including point-of-care ultrasound (POCUS) performed by midwives, can significantly reduce undiagnosed breech presentation in labour. This is welcome, as women find diagnosis of breech presentation in labour traumatic, regardless of the outcome.2 Although the considerable psychological impacts were not discussed, all should support the plan to increase safety, choice and personalised care through better antenatal detection of breech presentation.
However, the authors then assert that, “Short-term adverse perinatal outcomes, including [neonatal unit] admission and low Apgar scores, were significantly lower for the pregnancies with diagnosed breech presentation at term following a policy for screening by either routine third trimester scan or POCUS.” This was despite no evidence given that any neonatal outcome achieved a statistically significant improvement. Indeed, hypoxic ischemic encephalopathy (HIE) increased from 0.3% to 0.4% in the St Georges University Hospital (SGH) cohort. The authors then ran Bayesian log-binomial regression models mostly using data from a previous evaluation of the same intervention on a different population (Salim et al),3 falsely concluding that there was a high probability the intervention would reduce adverse outcome rates.
Oxford’s implementation data
The publicly available data for the Salim et al study (S1 Data. Study data set)3 indicate that eight cases of serious neonatal morbidity (HIE and/or death) occurred:
In six (75%) Oxford cases, the breech presentation was identified antenally. In 1/2 (50%) undiagnosed cases, a presentation scan would not have prevented the breech labour, which occurred at 37+2 weeks gestation. In both cases of death, the breech had been diagnosed clinically and the women had been seen in breech clinic. In two additional diagnosed cases, the breech service worked exactly as it was intended; two successful ECVs were performed. Nonetheless, HIE occurred following these cephalic births.
The total potential benefit in Oxford was a reduction of two cases of HIE and two less NICU admissions with Apgar <7 at 5 minutes without HIE, i.e. 44 versus 40 neonatal composite adverse outcomes in 1052 third trimester breech presentations, at a cost of 7,673 additional scans and 65 additional ECV procedures.
Norwich charity funding
Knights et al1 do not explain that Norfolk and Norwich University Hospital (NNUH) spent £100,000 of NNUH Hospitals Charity funding4 on handheld ultrasound scanners. The results in their cohort (Table 4) indicate two fewer neonatal admissions and one less case of Apgar score <7 at 5 minutes after implementation. Neither of these would have been considered a serious adverse outcome in the Term Breech Trial5 nor PREMODA study.6 Thus, there is no causative evidence of improvement, nor is this strategy is likely to prove cost-effective for implementation at scale.
St Georges’ specialist service
Knights et al failed to even look for confounding factors, let alone control for them – a serious source of bias in retrospective studies (see item 7 in the STROBE checklist, ‘Variables’).7 Yet, during their study time frame, and known to the authorship team, SGH also participated in a prospective multi-centre evaluation of physiological breech birth training, the results of which were already published in 2021.8 Both Knights and Mattiolo report a similar number of vaginal breech births, 64 (49 before and 15 after) and 90 (37 before and 53 after) respectively. Mattiolo et al also report outcomes for actual vaginal breech births. Among births where there was no attendant who had completed the enhanced training present, the severe neonatal composite adverse outcome rate was 5/69 (7.2%). Among births attended by someone who had completed the enhanced training, in the same settings, it was 0/21 (0%).
Between 2017-2020, overlapping with the implementation of the scanning programme, a specialist clinic and intrapartum care service for women requesting a vaginal breech birth were implemented at SGH.9 After 100 doctors and midwives had received a whole day’s training, the internal guideline was updated to include a physiological breech management algorithm.10 This was incorporated into monthly mandatory training to all staff, introducing substantial changes to vaginal breech birth practice. All obstetric trainees received half-day training. New joiners received the whole-day training repeated 6-monthly. By 2019, the rate of planned VBB had increased from 1.3% to 12.3% of all births in breech presentation.11 Internal audit of this service demonstrated substantial reduction in the emergency caesarean birth rate, from 42.9% to 24.8% of all births in breech presentation.11
The specialist service at SGH was discontinued when the breech specialist midwife (Spillane) relocated in 2020 and was not replaced. Nevertheless, the potential confounding effects need to be considered. When services invest in staff skill development, those effects extend beyond each individual birth.12
A specialist intrapartum service was also implemented at Oxford during the Salim et al. study,13 with the ‘dedicated on-call team’ for vaginal breech births publicly advertised on the hospital website.14 This is a significant difference in practice compared to most NHS units (except OptiBreech sites). Among the breech presentations >37 weeks with labour, planned vaginal breech births increased from 7.4% (12/162) to 17.6% (21/98) after the introduction of universal scanning. The provision of this team also appeared to improve the safety of the actual vaginal breech births that occurred.
Admission to NNU
Apgar <7 at 5
HIE
Perinatal mortality
Planned VBB
2/16 (12.5%)
0/16 (0%)
0/16 (0%)
0/16 (0%)
Unplanned VBB
7/42 (16.7%)
3/42 (7.1%)
5/38 (13.2%)
2/42 (4.8%)
Secondary analysis of publicly available data from Salim et al
The differences between planned and unplanned VBB are comparable to Mattiolo et al.8 Could the authors use these data in Bayesian log-binomial regression models to demonstrate the beneficial effect of implementing breech birth teams? We cannot assume that similar results would occur in settings that do not offer a similar service.
Summary
The opportunity to access a third trimester presentation scan remains important, especially for women planning an out-of-hospital birth. But women find it psychologically distressing and dehumanising to be unable to access skilled support for a vaginal breech birth, both antenatally and in labour.15–17 Unless an evidence-based plan for improving this support is in place, matters will never change. When we prospectively evaluated the implementation of breech teams,15 one in five participants transferred from their original booking hospital to access supportive care for a vaginal breech birth.18 Some of these women came from SGH (since this VBB service is no longer available) and NNUH (approximately three hours car drive from the nearest OptiBreech site). Further unanticipated risks are introduced for women whose babies are diagnosed as breech but who cannot access their preferred mode of birth locally. More inequalities are created among women for whom the required travel and self-advocacy is impossible.
Determining which interventions improve clinical and cost-effectiveness outcomes for term breech pregnancies requires properly powered, prospectively registered, randomised controlled trials with publicly available, pre-specified protocols and anonymised data sets. It is extraordinary that £100,000 of charitable money was spent on equipment alone, outside the context of carefully planned research, and without service user involvement in priority setting. This has merely resulted in a poor-quality publication and plenty of mass media soundbites.4,19,20 Currently, many NHS sites lack the funding for trained staff to offer all needed care options (ECV, VBB and ELCB) that are currently recommended in RCOG21 and NICE guidelines.22,23 Investing in staff and their skill development will achieve the same, if not better, results and should be the priority.
Investing in staff and their skill development for vaginal breech births will achieve the same, if not better, results than universal third trimester ultrasound scans and should be a priority. @optiBreech@MidwifeSpillanehttps://t.co/AVmvWbCFsJ
Knights S, Prasad S, Kalafat E, et al. Impact of point-of-care ultrasound and routine third trimester ultrasound on undiagnosed breech presentation and perinatal outcomes: An observational multicentre cohort study. PLoS Med. 2023;20(4):e1004192. doi:10.1371/journal.pmed.1004192
Lightfoot K. Women’s Experiences of Undiagnosed Breech Birth and the Effects on Future Childbirth Decisions and Expectations. DHealthPsych. University of the West of England; 2018. http://eprints.uwe.ac.uk/33278
Salim I, Staines-Urias E, Mathewlynn S, Drukker L, Vatish M, Impey L. The impact of a routine late third trimester growth scan on the incidence, diagnosis, and management of breech presentation in Oxfordshire, UK: A cohort study. Myers JE, ed. PLoS Med. 2021;18(1):e1003503. doi:10.1371/journal.pmed.1003503
Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. The Lancet. 2000;356(9239):1375-1383. doi:10.1016/S0140-6736(00)02840-3
Goffinet F, Carayol M, Foidart JM, et al. Is planned vaginal delivery for breech presentation at term still an option? Results of an observational prospective survey in France and Belgium. Am J Obstet Gynecol. 2006;194(4):1002-1011. doi:10.1016/j.ajog.2005.10.817
Vandenbroucke JP, Von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4(10):1628-1654. doi:10.1371/JOURNAL.PMED.0040297
Mattiolo S, Spillane E, Walker S. Physiological breech birth training: An evaluation of clinical practice changes after a one‐day training program. Birth. 2021;48(4):558-565. doi:10.1111/birt.12562
Spillane E, Walker S. Case study supporting continuity of care models for breech presentation at or near term. Pract Midwife. Published online 2019:36-37.
Spillane E, Winstanley C, Swer M. Breech. St George’s Hospital Practice Guideline; 2019.
Spillane E. St George’s Breech Clinic – Results. In: Physiological Breech Birth Training [Online]. Breech Birth Network; 2020. Accessed April 18, 2023. https://vimeo.com/486516151
Walker S, Parker P, Scamell M. Expertise in physiological breech birth: A mixed-methods study. Birth. 2018;45(2):202-209. doi:10.1111/birt.12326
Dasgupta T, Hunter S, Reid S, et al. Breech specialist midwives and clinics in the OptiBreech Trial feasibility study: An implementation process evaluation. Birth. 2022;00:1-10. doi:10.1111/birt.12685
Morris SE, Sundin D, Geraghty S. Women’s experiences of breech birth decision making: An integrated review. Eur J Midwifery. 2022;6(January):1-14. doi:10.18332/EJM/143875
Petrovska K, Watts NP, Catling C, Bisits A, Homer CS. ‘Stress, anger, fear and injustice’: An international qualitative survey of women’s experiences planning a vaginal breech birth. Midwifery. 2017;44(0):41-47. doi:10.1016/j.midw.2016.11.005
Walker S, Spillane E, Stringer K, et al. The feasibility of team care for women seeking to plan a vaginal breech birth (OptiBreech 1) – an observational implementation feasibility study in preparation for a pilot trial. BMC Pilot & Feasibility Studies. 2023;In Press.
Impey L, Murphy D, Griffiths M, Penna L, on behalf of the Royal College of Obstetricians and Gynaecologists. Management of Breech Presentation. BJOG. 2017;124(7):e151-e177. doi:10.1111/1471-0528.14465
A key element of OptiBreech Care is providing additional skilled and experienced staff at planned vaginal breech births (and unplanned ones too if we can manage it!) in line with the RCOG guidance.
We know this supports safety but traditionally it has been hard to achieve as the numbers of vaginal breech births may be few and far between, meaning limited experience and often limited or brief training. Most hospitals have < 1 hr a year for each of the common obstetric emergencies as part of their mandatory training, maybe less depending on each hospital’s rolling program of multidisciplinary skills and drills. Furthermore, expecting whoever is on and available to care for families having a Breech birth puts significant extra stress and strain on the on-call labour teams, often already pressured with complex scenarios and sadly short-staffed wards.
We often get asked- How to do the on-call elements of the OptiBreech care pathway work? Who will cover it? Everyone is doing enough already?!
Each of our current sites may operationalise its on-call systems slightly differently, however, the core elements are the same.
All sites need to create a Breech team- ideally, this consists of a mix of midwifery and obstetric staff willing to be on call for breech births. Ideally, each member will have had some prior experience of a breech birth (although this is not always possible). All members of the Breech team should have completed a recent OptiBreech study day, online or face to face and have had an opportunity to practice rotational manoeuvres via simulation before providing on call for births. We would expect team members to counsel women appropriately regarding experience and expertise as part of the initial personalised care planning.
We would advise that initially, the On-call Breech teams are smallish. You may start with one or two lead people who are first on call with a wider group of staff that want to gain experience and eventually join a full on-call system.
We have found that this is the most successful way to safely develop confidence and competence amongst the team whilst also building a sustainable service. Often when launching the team in a service that hasn’t previously been supporting vaginal breech births, it can take a while for any to come along. Too large a team means that it is hard for people to gain regular exposure and experience and in the long run it takes longer to develop expertise.
Structure and payment of on-calls
All sites have currently been opting for a voluntary on-call system. At my site, many of the team have other on-call commitments (as manager on call or perhaps homebirth on calls) so they try to combine the calls and to date, no one has minded being voluntary on call. If called into the birth, they are always added to the roster to ensure liability coverage and this has worked wonderfully for the intrapartum teams as they are always grateful to have an additional presence with expertise available to support the team!
We have found this system has been provided at no extra cost to the service and has increased staffing on shifts which would have otherwise been under the template. Two of our core Breech team midwives work full-time in Intrapartum services so they have been available often when needed just by the pure nature of their roles and shift patterns. Whilst it is difficult for clinical midwives to be on the call before a shift, both midwives work full time so are already working a significant number of shifts. If one of the families booked for a vaginal breech comes into labour, the labour ward team always work to release them to support with birth as required. Another of our team works as a specialist midwife Monday to Friday and again has often been available during her working hours to support Breech births when needed or if called out overnight is able to rearrange her day as needed.
You will require one lead practitioner who can coordinate the Breech team and ensure appropriate care and on call coverage. Usually this will be the midwife leading the Breech Clinic but it could be an alternative depending on your context. The lead practitioner will provide details of the on-call service and then arrange with the wider team any dates they can’t cover.
In some sites, Breech teams prefer for women to contact them directly when they are in labour and the on-call team alerts the rest of the service, in other teams, the families will contact the triage service as per usual and then the Breech team will be alerted. Your system will depend on how your team is developed and your current on call working practices.
When women are in labour, other team members are invited to attend for additional experience and support, again this is facilitated voluntarily but we have found no problem with people wanting to be involved.
What if we have no one available or we don’t make it in time?
Sites need to make a realistic effort to try and support this as we know it improves safety outcomes and it is the core process outcome for the Optibreech care package but also women are honestly and realistically counselled. If no one from the team is available ( we know last minute dramas can happen) the care would fall to the rostered labour ward team and if they have limited experience in vaginal breech birth, they would counsel them as per their practice, which would usually be to recommend a cesarean birth.
Results from the feasibility study showed that across all sites a Optibreech team member was present for 87.5% of planned vaginal Breech Births.
We have found vaginal breech births have risen from 2 in 2021 to 10 successful (18 planned) last year with no admissions to special care and we have around 1/2 women a month planning a vaginal Breech birth. As our numbers have increased, we have been able to support more midwives and doctors able to lead the care and meet the full OptiBreech proficiency criteria. We are now considering implementing a more traditional on-call system to cover the whole month.
** A key aspect of care is the OptiBreech team member is addition to the case midwife. This is a pivotal part of the safety mechanism. The OptiBreech team member supports situational awareness, liaison with the wider MDT and ensures prompt action is taken if concerns arise**
Other OptiBreech sites operate similar variations to the above model, partly depending on their Breech birth numbers, initial expertise in the team and also taking into consideration individual contexts and staffing models.
Key aspects required for a Successful Optibreech On-Call Team
Motivated individuals with a desire and flexibility to work this way
A lead clinician to coordinate care, on-call availability and liaison with families
A small group of staff initially to enable ongoing enhancement of competency- this group could be expanded as numbers and confidence grow.
Read why our collaborators would like to help extend the provision of OptiBreech care by participating in a cluster trial.
As we prepare our funding bid to scale up OptiBreech care around the UK and evaluate it in a stepped wedge cluster trial, we have invited NHS sites to formally express an interest in collaboration. We are pleased to share some of our collaborators and the reasons they are joining this trial.
Walsall Healthcare NHS Trust
Lead: Joselle Wright, Head of Midwifery
“We are a smaller DGH with 3700 births, smaller units often do not get the opportunity to participate in these amazing research studies. This would be a great opportunity for our women.”
Shrewsbury and Telford NHS Trust
Lead: Dr Olusegun Ilesanmi, Consultant Obstetrician
‘Research within our Trust is important as this enables us to ensure we provide up to date evidence based safe care, with Women & their babies at the centre. The Opti Breech Study promotes informing Women about their options and to plan their care with them rather than making decisions about them, as well as improving our expertise, knowledge, and staff development. We look forward to giving Women within our care the opportunity to be part of the Opti Breech Study’
Maidstone and Tunbridge Wells NHS Trust
Lead: Charlotte Gibson, Consultant Midwife
Maidstone & Tunbridge Wells OptiBreech Team-to-be a the RCOG, May 2023
‘This is an exciting opportunity for us to support women’s health research which will positively impact those who provide care, the service we are able to offer and ultimately optimise health and well-being outcomes for those we care for. All with the added and far-reaching benefit of growing and strengthening our clinical research culture and capabilities within our service, community and beyond. It was from women’s and families lived experiences that led us to embark on setting up a Breech Birth Faculty. Our aim is to build the capabilities and confidence within our workforce to support safe and personalised care for those who have a breech baby at term. Collaborating with the Opti Breech Trial will be fundamental in achieving this aspiration.‘
West Hertfordshire Teaching Hospitals NHS Trust
Lead: Claire Church, Consultant Midwife
“We would like to get involved in Optibreech so that we can offer a comprehensive, standardised service to our women and birthing people with breech babies which ensures that they are all counselled in the same way and given informed choice regarding their options. We also want to provide our staff with the skills and competencies to support our women and birthing people with their choices and feel confident in doing so”. – (Clare Church. Consultant Midwife)
North Tees and Hartlepool NHS Foundation Trust
Lead: Kirsty Farrington, Sharon Gowans and Julie Woollaston – Research Midwives
‘We are really excited to be involved in this research! It is a great opportunity to not only work towards delivering evidence-based care for women but also to develop skills and build confidence within the whole maternity workforce.’
NHS Lothian, Royal Infirmary of Edinburgh
Leads: Rosemary Townsend and Andrew Brown, Consultant Obstetricians
Wirral University Teaching Hospital
Lead: Consultant Midwife Angela Kerrigan
It will be fantastic to be involved in the Optibreech trial as it will offer additional skills to our staff to enable us to provide an enhanced service to women who present with breech presentation at Term through the Optibreech collaborative care pathway. This is really a exciting trial to be involved in that has the potential to positively influence the care of women with babies presenting breech at Term.
Wrightington, Wigan and Leigh Teaching Hospitals NHS Foundation Trust
These principles underpin the new JRCALC guidance on breech birth, due to be published next month. Ambulance clinicians, keep your eyes out 👀 #Breech#JRCALChttps://t.co/jCkvpcbs9j
Looking to engage with research, develop your critical appraisal skills and sharpen your own writing? If you have academic research training, consider becoming involved in peer review.
In my role as Researcher in Residence at Imperial College London, I support clinical NMAHPPs (nurses, midwives, allied health professionals, healthcare scientists, pharmacy staff and psychologists) to develop careers in research. As part of this, I have begun recommending midwives with Masters or PhDs as peer reviewers, when I am asked to review an article that I know fits their clinical or methodological areas of interest. I also offer support through this process. This fairly simple activity seems to have really hit a chord with clinical midwives who are looking to become more research-active, so I want to share it with others who are supporting clinicians to engage with research.
How the peer review process works
First, let’s de-mystify how people become involved in peer review activity. When you submit an article for publication, this is all done on-line. As part of this process, you enter your personal details, including (this is important!) your areas of interest and expertise. Even if your article is not accepted for publication, your details are retained on the journal’s database. When an assistant editor does a search for peer reviewers with an interest in, say, ‘breastfeeding,’ if you have listed this as one of your areas of interest/expertise, your details will come up in the search results. They are likely to ask the ‘big names’ first, people who have published a lot in this area. But top academics get many more peer review applications than they can accept. So, eventually, you will get asked to peer review in your area. Of course, if you have published as well, this will happen sooner.
For example, in 2012 I submitted a conference report to the British Journal of Obstetrics and Gynaecology (BJOG) because I thought people should know about the exciting, international changes that were beginning to happen around the way breech births were managed. It was rejected within 24 hours (ouch!). But soon, I started being asked to review articles in this area – probably due to very few other people listing ‘breech presentation’ as their area of interest. BJOG has still never accepted one of my academic articles, but by 2016, I was awarded a certificate as one of their top 50 reviewers! In 2018, I was rated a top 1% reviewer in Clinical Medicine by Publons peer review tracker, part of Web of Science. The insight I have gained into the publication process through peer review has been invaluable.
The other way you may get asked to peer review is because someone who is declining to peer review has nominated you as an alternative. Usually, senior academics will nominate more junior academics. This is what I have been doing for clinical midwives who hold at least a Masters at Imperial, provided I know their areas of interest. Again, if you accept the invitation, your details will be in the system, and you will likely receive future invitations.
You can also write to the editor of a journal you are interested in, with your CV, and offer to do peer review.
Benefits of doing peer review
Once they finish a further degree, clinicians often start to feel detached from the academic research world. Doing peer review is one way to stay engaged and be inspired by others’ work. It helps you develop critical appraisal skills. You observe how successful articles are structured, and why, until it becomes second-nature when you begin to plan your own work. You gain exposure to other methods and methodologies being used to answer research questions in your field. And you begin to see gaps in knowledge or need for further research, which may help you define a project you would like to pursue yourself.
Midwife in training Jacana Bresson
If your professional aims include applying for fellowship or research funding, peer review activity is regarded favourably on your CV. You can automatically upload your peer review confirmation e-mail to the Publons website, just by forwarding it. And you can then simply list your public peer review profile on your CV – here’s my Web of Science profile, including peer review.
Personally, I also enjoy the feeling that I am influencing what gets published and becomes part of our evidence base. For example, I have reviewed innumerable articles which either directly concern midwifery practice or have the potentially to significantly impact it, yet the research team does not include a midwife. I have consistently given the feedback that, in the future, it should; and that this should be acknowledged as a limitation in the discussion. By remaining present in the sphere of peer review, midwives and NMAHPPs can make a genuine difference.
Support with this process
For NMAHPPs working at Imperial, I can help you become involved in peer review for the journals you read. If you would find it helpful, I can support you to complete the review, so that you feel confident returning your critical appraisal. The involvement of another person needs to be declared to the editor, as the peer review process is otherwise confidential, but this is acceptable when less experienced reviewers are receiving support.
Nimisha Johnstone, @OptiBreech PPIE lead, shares women’s views of why it’s important we help babies to start breathing with the cord intact when needed. @NIHRinvolvement
In autumn/winter 2022, the OptiBreech research team spent time developing a research proposal for a study to investigate the implementation of bedside resuscitation for breech babies who require breathing assistance at birth. In my role as a PPI leader with the OptiBreech trial, I sought input from breech presenting mothers and birth workers through small group interviews.
I am the mother of a baby who presented breech at the end of pregnancy. I planned a vaginal breech birth and agreed to allow my birth data to contribute to the OptiBreech study in 2021. Since then, I have become involved in enabling other mothers of breech-presenting babies to become involved in shaping the evolution of this research.
Birth Experience
I spoke with 7 women with a breech presentation at term and 1 doula over video calls in groups of 2. We started by sharing our breech birth experiences and the themes of lack of choice and lack of confidence in birthing professionals echoed across all interviews. The need for support towards a physiological breech birth was not met in many of the experiences resulting in a lack of choice and feelings of coercion towards a c-section. They reported a confidence in their body’s own ability to birth breech, but a lack in the birthing professional’s ability to confidently support them.
The mothers were aware of optimal cord clamping and the benefits, however, similar to the women in our OptiBreech studies, they had reported feeling let down because the cord was clamped immediately, despite stating their wishes on their birth plan. They also reported not being made informed as to why the cord was clamped immediately.
Some of the mothers also reported their baby being taken to a resuscitation table out of sight without being informed. Seeing their baby on the resuscitation table led to feelings of self-doubt, guilt and questioning whether they had made the right choices.
Is this research proposal important and relevant?
The research proposal aims to answer two questions:
What are the outcomes for mother and baby for term breech pregnancies within the services offering optibreech care?
And can bedside stabilisation and/or resuscitation following vaginal breech births be successfully implemented with provision of a bedside unit and staff training?
About 1:5 babies born after a vaginal breech birth need some help to start breathing, and about 1:10 are transferred to a neonatal intensive care unit after the birth. We feel we can reduce this to 1:5 (the UK national average for all births) if our specialist teams are able to provide help next to the mother. This will result in better long-term outcomes for the baby. Families have better experiences if they are not separated from babies, during resuscitation or after. Women in our OptiBreech studies have reported feeling let down because in most births where the baby appeared to need help, the cord was cut immediately, despite OptiBreech and UK Resuscitation Council guidance.
All mothers strongly support the research proposal and believe optimal cord clamping and keeping the baby near to them immediately post-birth is hugely important. Some mothers reported feelings of confusion as to why this did not happen in their experience because they felt it was quite obvious that babies should be near their mother immediately post-birth, therefore were supportive of having a bedside unit so that they could always see their baby if they needed resuscitating.
Mothers reported doing more research on neo-natal death rates resulting in them feeling less informed around the need for resuscitation. Sharing this scenario before birth would help to keep the mother informed around a potential post-birth scenario as well as the need to keep the mother informed in real-time should a resuscitation unit be needed.
Language
The importance of the use of language was highlighted, in particular the use of the word “resuscitation” did not resonate well with some of the mothers as it can lead to negative connotations such as not being able to breathe or death. There was an understanding that the resuscitation table is also used for clearing the lungs and or for simply checking the baby and therefore the word “resuscitation” should be carefully considered when speaking to mothers to avoid panic. “Transition” was one replacement word suggested, however, there were mixed responses to this word as some felt it wasn’t specific enough and needed explaining whereas others responded positively saying it’s a mid-way point. There will need to be further consideration around the use of language and the most appropriate terminology to use.
Thank You
We ended the session by sharing our motivation for joining this PPI meeting and learnt that mothers wanted to be a part of the driving force behind normalising physiological breech birth, and to avoid other mothers and birthing people feeling like they have no other option.
I would personally like to say a huge thank you to those who participated in this PPI meeting, it was a pleasure meeting each of you. We value your thoughts and comments to improve on the design of our study to better our research.
Expressions of interest are invited for sites to collaborate on an HTA funding bid for a stepped wedge cluster trial of OptiBreech care.
We are aiming to submit a funding proposal in August 2023 and if successful, plan to begin work on the trial in summer 2024. We hope to include sites from Scotland, Wales, Northern Ireland and England, with a preference for sites outside of London that benefit from participation in research less frequently.
We expect to part-fund a developmental breech specialist midwife post. This is a highly sought-after position that is likely to attract external applicants and contribute to staff retention.
Participating sites get unlimited free in-person and on-line training that has been fully evaluated in NHS settings,* support with implementation and involvement in OptiBreech community of practice. * This is the same training offered through the RCOG.
Women would retain choice of ECV/no-ECV and mode of birth. We expect a modest increase in planned vaginal breech births in most settings.
Kate Walker, Clinical Professor of Obstetrics, University of Nottingham
Debra Bick, Professor of Clinical Trials in Maternal Health, Warwick Clinical Trials Unit
Kate Stringer, Consultant Midwife and Implementation Lead, Surrey and Sussex Hospitals
Rosemary Townsend, Senior Clinical Fellow in Obstetrics, University of Edinburgh
Andrew Brown, Consultant Obstetrician and Skills Training Lead, NHS Lothian
Amy Meadowcroft, Breech Specialist Midwife and NIHR PCAF, Oldham
Siân Davies, Perinatal Psychologist and PPIE Lead
What is OptiBreech collaborative care?
OptiBreech care is a new care pathway for delivering standard care to women and birthing people pregnant with a breech-presenting baby at term. This population is defined as: breech presentation at birth, or at any scan from 35+0 weeks or where a successful external cephalic version (ECV) has been performed.
Phase 2 @optibreech is looking for new sites! See EOI for more info- https://t.co/8n9uZRMSeL We are keen to engage sites with varying demographic and size across 🇬🇧 Funding/training/implementation to set up Breech Clinic and services. DM for 1:1 or more info. Happy to discuss
The service is provided through a dedicated clinic, co-ordinated by a breech specialist midwife, working collaboratively with a breech lead obstetrician. All management options are offered – external cephalic version, vaginal breech birth and elective caesarean birth. ECV attempts are provided by clinic staff in a same-day service where required. Intrapartum care for vaginal breech births follows the OptiBreech physiological breech birth guideline, developed by the OptiBreech Collaborative. The breech lead midwife and obstetrician lead on training throughout the service, including mandatory updates and simulations. The specialist midwife also co-ordinates a continuity of care service, so that whenever possible planned breech births are attended by a member of the team with full OptiBreech training and experience managing complications. Members of the team are also part of an extended OptiBreech community of practice, which provides regular practice updates and opportunities for reflection as they develop competence and expertise.
How does this differ from standard care?
This is a new way of organising care and training for breech presentation at term. Current standard care is characterised by a lack of standardisation and adherence to national guidelines from the RCOG(1) and NICE(2). OptiBreech care promotes standardisation for optimal outcomes. The vaginal breech birth training that is provided is the same training offered on the RCOG Labour Ward Management course, RCOG Vaginal Breech Birth study days and Royal Society of Medicine Maternity and Newborn Forum, which led by clinical members of the research team.
These principles underpin the new JRCALC guidance on breech birth, due to be published next month. Ambulance clinicians, keep your eyes out 👀 #Breech#JRCALChttps://t.co/jCkvpcbs9j
Why do we think a cluster trial is appropriate now?
There is strong evidence current standard care pathways do not provide consistent access to all options national guidelines recommend,(3,4) nor do they provide adequate training opportunities for younger obstetricians and midwives.
OptiBreech collaborative care is a pathway developed with significant input from service users and clinicians. It is highly acceptable to women and birthing people, regardless of their care choices or ultimate mode of birth.(5)
Feasibility work has included two NHS training evaluations,(6,7) an observational implementation evaluation and a pilot trial. All three have demonstrated better outcomes compared to standard care for vaginal breech births. For example, the neonatal serious adverse outcome rate for women planning a vaginal birth has been less than 1%, compared to 5% in the Term Breech Trial,(8) and 7% for actual vaginal births in standard care births included in our training evaluation.(7)
The pilot trial demonstrated that women have access to all three guideline-recommended options within the OptiBreech care pathway, but not within standard care (see below).(9)
Pilot trial results: More women planned a VBB when randomised to OptiBreech Care (23.5% vs 0, p = .003, 95% CI =.093,.378). Women randomised to OptiBreech care had: lower rates of cephalic presentation at birth (38.2% vs 54.5%), higher rates of vaginal birth (32.4% vs 24.2%), lower rates of in-labour caesarean birth (20.6% vs 36.4%), lower rates of neonatal intensive care (5.9% vs 9.1%), and lower rates of severe neonatal morbidity (2.9% vs 9.1%). Within the entire cohort, breech presentation on admission to labour/birth (n=44), compared to cephalic presentation (n=38), was associated with: lower levels of neonatal admission (2.3% versus 10.5%), lower levels of severe neonatal morbidity (2.3% vs 7.9%), fewer maternal admissions to HDU (4.5% vs 7.9%) and less severe maternal morbidity (13.6% vs 21.1%). Outcomes for non-British and non-white women were also better than participants from white British backgrounds, which reassures us this service is accessible to minoritised participants. Randomisation was stopped in June 2022 on the advice of the steering committee, at 68 women randomised rather than the planned 104. It was clear 1:1 randomisation would not enable us to compare outcomes for VBB because women were not choosing to plan a VBB within standard care.
We know that the model enables access to a guideline-recommended care option (VBB), but we do not know how this will affect outcomes. A definitive trial that is powered on serious adverse neonatal outcomes is urgently needed and could lead to the implementation of OptiBreech collaborative care across the NHS.
What outcomes do we expect to improve with OptiBreech care?
Based on the results of our feasibility work and the available literature, we think that the rate of serious adverse neonatal outcomes (including death, HIE, admission to the neonatal unit >4 days) is about 4.5% for the entire cohort of term breech babies within standard care, as defined above. We think we can reduce this by about 40%, to 2.7%. This is the primary outcome we are seeking to improve.
We also think that OptiBreech care will be more cost-effective and reduce the rate of emergency caesarean birth.
How do we think OptiBreech care will do this?
We expect up to 1-2 women per month at each centre to plan a vaginal breech birth, with no increase in adverse outcomes for these babies. (Note: This is an estimate of what might happen when services are delivered in this way, but there is no target VBB recruitment rate. Women’s choices remain the same.) Your site will implement the new care pathway for women booked at your service but will not be promoted as an OptiBreech referral site.
Based on available evidence and our feasibility work, we expect a reduction of 0.9% of serious neonatal outcomes will come from increasing skill levels throughout the service, learning from these planned events, and improving mandatory skills training to bring it in line with the most current evidence. We think this will help prevent adverse outcomes in unanticipated vaginal breech births.
In multiple audits and our pilot trial, we have also observed that within this model of care more women choose an elective caesarean birth, and the emergency caesarean birth rate declines. This will result in 0.9% additional improvement in neonatal, maternal and economic outcomes.
How will we evaluate this?
We will evaluate this in a stepped wedge cluster trial, including twenty sites over three years. If your site is chosen to participate, you will implement the care pathway at a point during the three years determined through randomisation. Our research team will analyse outcomes for women receiving care at the sites prior to and after randomisation.
What support would participating sites receive?
If you are one of twenty sites chosen for this trial, your hospital will receive unlimited free physiological breech training. This training is currently provided through the RCOG at a cost of over £360/person. We will train any members of your team you would like to receive full training. We will also train your skills trainers to deliver updates through standard mandatory training activities and periodic simulations.
At this point, we hope to be able to fund one half day per week of a Band 7 breech specialist midwife developmental post. This person will be a current Band 6 ready to step up to greater leadership within the service. They would need to be in post for between one to three years, with associated funding between £12,126 and £36,379, depending on your site’s starting point in the trial. They would be supported by senior members of your team to develop into a specialist. Your breech specialist midwife will also collect the data for the study, and the time for this will also be funded through the CRN; this is likely to be approximately 0.1 WTE, depending on the size of your service. This is a desirable post for the right person, which we anticipate will contribute to staff satisfaction and retention, in addition to developing your breech service.
We would provide you with a comprehensive job description, guideline and training resources, operational during the time your site is ‘live’ on the trial. This guideline has been developed by the OptiBreech Collaborative, clinicians who have led the first stages of feasibility work for this trial.
We would provide you with support during the implementation period from an experienced member of our team who has successfully implemented the service we are testing. And we would provide support through our community of practice activities for all members of your team who wish to participate. These include regular practice updates, case reviews and opportunities for reflective supervision with clinicians experienced in supporting physiological breech births. As many new sites will have limited recent experience supporting planned vaginal breech births, this will be re-introduced in a controlled and supported way.
Why else should you consider participating?
If this trial has a positive result, the OptiBreech collaborative care pathway will likely become the standard of care, and you will have already implemented it. If the trial does not demonstrate an improvement in outcomes, your team would still have acquired significant experience in the management of vaginal breech births, which may still bring beneficial skills and knowledge into your service.
Where can I read more about the research supporting OptiBreech care?
Please complete this form with your name and contact information. We will contact you with more information about requirements for site selection.
References
1. Impey L, Murphy D, Griffiths M, Penna L, on behalf of the Royal College of Obstetricians and Gynaecologists. Management of Breech Presentation. BJOG [Internet]. 2017 Jun;124(7):e151–77. Available from: http://doi.wiley.com/10.1111/1471-0528.14465
4. Roy R, Gray C, Prempeh-Bonsu CA, Walker S. What are women’s experiences of seeking to plan a vaginal breech birth? A systematic review and qualitative meta-synthesis [version 1; peer review: awaiting peer review]. NIHR Open Research 2023 3:4 [Internet]. 2023 Jan 20 [cited 2023 Jan 21];3:4. Available from: https://openresearch.nihr.ac.uk/articles/3-4
6. Walker S, Reading C, Siverwood-Cope O, Cochrane V. Physiological breech birth: Evaluation of a training programme for birth professionals. Pract Midwife. 2017;20(2):25–8.
8. Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. The Lancet [Internet]. 2000/10/29. 2000 Oct 21;356(9239):1375–83. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11052579
9. Walker S, Spillane E, Stringer K, Trepte L, Davies SM, Bresson J, et al. OptiBreech collaborative care versus standard care for women with a breech-presenting fetus at term: a pilot parallel group randomised trial to evaluate the feasibility of a substantive trial nested within a cohort. In peer review. 2023;
Stakeholder Engagement
Funding for the Breech Specialist Midwife post at Band 7
The activities performed in a breech clinic are not new. ECV, VBB and caesarean birth are all guideline-recommended choices and RCOG-recommended auditable services. Offering them through a dedicated clinic with a small teams with a high level of skill and experience is new. The change management required to shift these tasks into a dedicated clinic, develop the skills to run the clinic and manage the service so that staff who need training are able to rotate through the clinic – this is the ‘new’ thing that requires extra organisational time and incentives. But once in place, it helps all of the basic services run more efficiently, at a higher standard.
Few opportunities for progression – Discussions with midwifery managers and staff outside of the southeast of England indicated there are few opportunities for midwives to progress in their careers to a senior midwife post. For this reason, we will require the appointment to be at least a beginning Band 7. We want the post and the project to offer greater opportunities to health boards and hospitals that benefit from participation in research less frequently.
Not enough research staff – The breech specialist midwife will be seconded to the research team for at least 10% FTE (half a day a week). The funding will this will come from the Clinical Research Network (CRN) pots that fund all research midwives and nurses. Collecting service data also contributes to the breech specialist’s growing expertise. By the end of the project, they will have additional transferrable skills to remain active in clinical research, either through further work as a research midwife or by pursuing a clinical academic role. It also offers the specialist increased flexibility in their working patterns. Sometimes, a clinic day is not full of breech-presenting babies; data can be collected. Sometimes, there is a late diagnosis of breech presentation requiring urgent counselling; or a birth occurs overnight before a research shift; data collection can easily be rescheduled.
Will anyone be willing to take on the role? Managers worried that the post would require someone to take on a lot of responsibility and that their staff are often very junior due to staffing shortages. They often expressed worry that they might not find someone willing to take up the post. However, often in the same conversation, someone was simultaneously offering to fill the post or identifying someone who would be very keen to ‘own’ the project locally. Our experience is also that experienced junior staff often ‘grow’ in this position, as it gives them an opportunity to expand their skills and autonomy with support. However, due to this worry, we will work with sites who express an interest to ensure they have identified someone who is willing and able to take up the position in advance of confirming them as a collaborator on the funding bid.
Most obstetric staff who expressed an interest were very keen to participate but worries that they were not seeing sufficient numbers of women planning a vaginal breech birth to make it worthwhile.
There is no VBB target. We have reassured sites that this study is NOT about promoting vaginal breech birth, and there is no minimum target of VBB numbers to achieve. If no one plans a VBB, and one-month follow-up surveys indicate that they felt well-informed and supported, with all choices available, there is no problem! If on the other hand, follow-up surveys indicated women are meeting resistance when they attempt to plan a VBB, we would work with sites to address this.
“There are many barriers within our service.” Multiple obstetricians who were otherwise keen to support women’s choice to plan a VBB described the same barriers within their service:
Not all women eligible were referred for an ECV attempt. Many were just encouraged to plan a caesarean section. (This aligns with available systematic review evidence, our interview data and our PPI feedback.)
When women chose to plan a VBB after a failed ECV, they often wanted to return to talk about it a bit more. But they returned to their named consultant’s clinic and were discouraged, so many abandoned their hope to plan a VBB. (This aligns with available systematic review evidence, our interview data and our PPI feedback.)
Some women felt confident to plan a VBB with appropriate counselling, but when they arrived in labour, it was very clear that the clinical team on duty were not supportive. Often, they would find any excuse to recommend an emergency caesarean early in labour, eg. suspecting a ‘footling breech’ at 2 cm when previous scans have indicated an engaged pelvis. The few women who continued to plan a VBB often ended up feeling very let-down and disappointed with the service. (This aligns with available systematic review evidence, our interview data and our PPI feedback.)
Because of this, obstetric staff often felt frustrated that, although they wanted to participate, it might not be possible in their setting.
This is the problem in almost ALL settings. You are not alone! The standard care pathway is not working in most settings for precisely these reasons. That is why our proposed intervention is a care pathway intervention. Even if we have improved the safety of VBB, if there is no way for women to benefit from this, and no way for staff to learn from it, nothing will change. This is the problem our ‘intervention’ (a dedicated clinic and service, co-ordinated by a breech specialist midwife) is designed to improve. Once you ensure that women receive consistent counselling and continuity of care, you can begin to benefit from improved training and cultural change.
If you would like to offer feedback privately, you can contact our PPI Lead, Siân Davies. Siân has lived experience of breech pregnancy, is a perinatal psychologist by training, and has additional training in trauma-informed care. Our PPIE team also includes Nimisha Johnstone.
We held two online engagement events in March 2023. These were attended by four women with lived experience of breech pregnancy and planning a vaginal breech birth and two midwives. Additional feedback was obtained via social media channels and a survey. This was how we advertised them:
Monday, 6 March, 2-3.30 pm — via Zoom
Tuesday, 14 March, 6-7.30 pm — via Zoom
Events are open to women and birthing people and maternity care providers throughout the UK.
Below is a description of one of the studies we would like to do. We invite anyone to comment on the study design and description (online survey; will remain open until early May 2023), particularly families that have had a breech-presenting baby within the past 5 years in the UK. We can answer any questions you have during the engagement meetings, or you can contact us via e-mail using the form below.
OptiBreech ECV or no-ECV trial
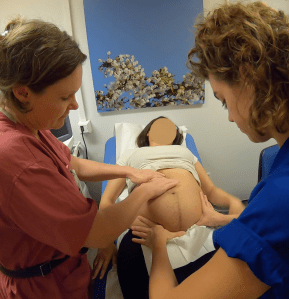
ECV with midwives Shawn and Lucia Pederiva (shared with permission)
Approximately 1:25 babies is breech at the end of pregnancy, positioned head-up instead of head-down in the womb. Current standard care is to offer women an attempt at turning the baby to head-down, through pressure on the abdomen (external cephalic version, ECV). However, this procedure is only successful 50% of the time and some women prefer not to try it.
OptiBreech care is delivered through a dedicated clinic, co-ordinated by a breech specialist midwife collaboratively with a breech lead obstetrician. It includes care during labour for women and birthing people who plan a vaginal breech birth (VBB). In our first study of OptiBreech care, women who planned a VBB without a prior attempt at ECV (no-ECV) had higher rates of vaginal birth. In our small trial, women receiving OptiBreech care had higher rates of vaginal birth and better outcomes compared to women receiving standard care, including all modes of birth.
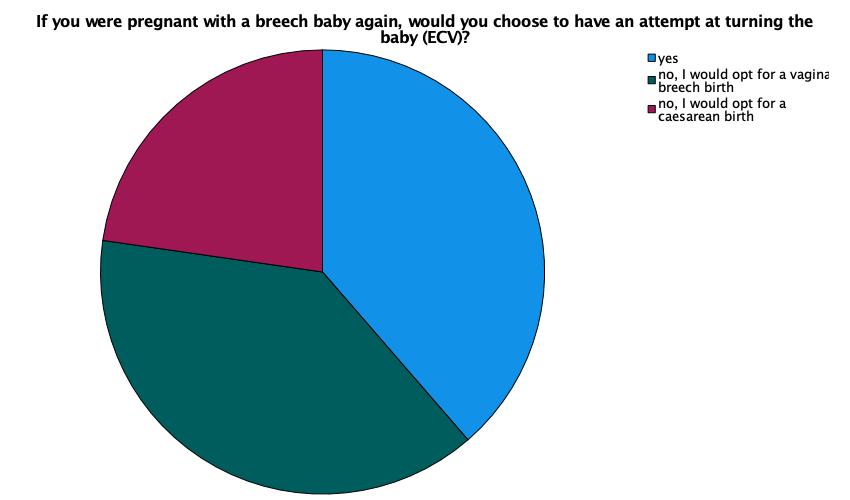
In surveys one month after birth, 60% (29/48) of OptiBreech participants said they would not attempt an ECV in a future pregnancy. OptiBreech clinicians are also uncertain whether trying to turn the baby provides additional benefits, including more vaginal birth and less overall healthcare costs, compared to no-ECV within OptiBreech services.
The thoughts of 48 women following breech pregnancies on ECV if they had another breech baby. Note: This is a current snapshot of our responses and may change. Also, more women in this sample had unsuccessful ECVs, which will influence views.
The aim of this research is to determine if attempting to turn breech babies head-down (ECV) offers additional benefits, compared to OptiBreech care with no-ECV.
The design is a randomised controlled trial. Participants will be women over 36 weeks of pregnancy who wish to plan a vaginal birth regardless of whether their baby remains in a breech position. Those who choose to participate will be allocated by chance (randomised) to one of two options.
The ‘standard care’ group (the control) will have an ECV attempt. If unsuccessful, the person will plan a VBB with OptiBreech care. The experimental group will be no-ECV; these will plan a VBB with OptiBreech care. We will compare these two groups to determine whether the vaginal birth rate differs between them and whether care for one group costs more than care for the other.
Our stakeholders, OptiBreech clinicians, participants and Patient and Public Involvement group members, have highlighted the need for this research. While some women may continue to prefer an ECV attempt, others would prefer not to have one if additional benefits are not clear. This could potentially save healthcare resources or alternatively reassure us that ECV is still important in OptiBreech contexts.
This research is aimed at influencing national guidance. We will work with the Royal College of Obstetricians and Gynaecologists to ensure this happens. We will also share our results with participants and the public through publications and our engagement website, optibreech.uk.
Dr Shawn Walker, OptiBreech Chief Investigator
Stakeholder feedback and questions
From our first engagement event:What happens if someone gets randomised into ECV and they didn’t want this and decides not to go ahead with the plan?
Ideally, we would like people to decide if they will be happy to have an ECV and/or a planned vaginal breech birth before agreeing to participate. However, we respect everyone’s autonomy and ability to withdraw from research interventions. We would continue to include the person’s results (with consent) and would take account of the change of plan in the statistical analysis. The reality of breech care is people often do change their minds, both about ECV and about VBB.
Could woman opt in for ECV or no ECV themselves?
Yes, but not if they are participating in the trial. Randomisation reduces bias by removing the element of choice from both women and clinicians. So participants would need to decide if they are happy to give up that choice, and accept ECV or no-ECV according to the way they are randomised.
If women decide NOT to participate in randomisation but still wish to plan a vaginal breech birth, they will be invited to participate in the observational cohort arm of the study. This option may or may not be available to women booked externally to participating centres, depending on whether OptiBreech care is considered the standard of care or an experimental treatment (on-study only) within that hospital. It may also depend on the team’s capacity.
From our first engagement event:If someone has had a previous caesarean birth but they would like this birth to be vaginal, could having an ECV cause issues because of the previous birth mode i.e. ruptured membranes etc?
From our first engagement event (midwife stakeholder):Computer randomisation does reduce clinical bias, however would the clinical midwife involved in the study increase bias by them recruiting participants?
Yes! This bias could go either way. Sometimes people are not recruited because, for example, the clinician does not feel it would be appropriate to offer them one option or another. Sometimes there is confusion about inclusion criteria so that women at moderate risk (eg. one previous caesarean birth) are not offered the opportunity to participate. To counter-act this potential source of bias, we will create posters for recruiting sites to display in areas where women receive antenatal care, providing them with a neutral point of contact, such as a research midwife. We will also share information on this website about how women can self-refer onto the study. This will enable as many women to access the research as possible and limit the bias from clinician selection.
From our online survey:How do people get consented to the randomisation?
Great question! The health care professional who informed the person about the research would offer further written information and the opportunity to ask questions. Then we would ask for consent, usually online, directly onto our database via the participant’s personal e-mail, which is also used for follow-up surveys. Alternatively, consent can be taken via written signature on the same consent form, on paper. An example of the participant information sheets and consent forms we currently use can be found on our Information for Women and Birthing People page.
In some settings, OptiBreech team care has become the standard of care. In others, it is still considered an experimental care pathway within the service, with the service funded by clinical research network funds. In the latter case, OptiBreech care would only be available through participation in the research.
From our online survey:I’d want more information about what OptiBreech is, but appreciate this may confound the research.
We want participants in this research to have a very clear idea about what OptiBreech Care is. We explain it in our participant information sheets, which are similar to those we would use in this research. These can be found on our Information for Women and Birthing People page.
Questions about breech birth at home
From our online survey:
What about those who wish to birth at home?
I suspect the research will take place in hospital, but that hasn’t been made clear.
Supporting women in any location.
Any data on VBB home birth.
Our OptiBreech Guideline recommends birth in hospital, within an obstetric unit. However, this is not required. We neither require women to give birth in hospital nor require local OptiBreech teams to attend births outside of the hospital. As with most standard breech criteria, our approach is to observe rather than to control. Women on our study have chosen to give birth in the full range of settings available to all other women, although sometimes the ability to do this is affected by local staffing constraints. It is too early to offer information about how place of birth influences results for OptiBreech care.
From our online survey:Does this include footling breech presentation? As all basic literature I have found suggests c section always offered with these.
You are absolutely correct that this has been the traditional approach. But our approach is to base all of our guidelines on evidence.
Our view of the literature is that ‘footling’ presentation is poorly and inconsistently defined, making it difficult to draw conclusions about risk. Increased risks pre-term (before 37 weeks) are clear, but the available literature indicates that non-extended (non-frank / both legs straight beside the body) presentations may actually have BETTER outcomes at term. We therefore do not recommend a caesarean birth unless the feet are presenting and the baby’s pelvis is not engaged, eg. positioned above the inlet to the maternal pelvis. We call this position, ‘standing.’
When baby’s legs are flexed (bent), we counsel women about the increased risk of a cord dropping down in labour, which would require a caesarean birth if it happened. And we explain the clinical uncertainty, eg. we do not know for certain whether there is increased risk or not.
Instead, we collect data about what position baby’s legs are in during antenatal scans and what position the legs are in at birth, and of course what the ultimate outcome is. In that sense, yes, footling breech presentation is included, and not excluded, from this research.
How will you record babies that turn by themselves without an attempted ECV or after a failed ECV?
In the OptiBreech database, we record: 1. Initial plan after first counselling – ECV/VBB/CB; Result of all ECVs planned – not done (and reason)/successful/unsuccessful
Will you allow a 2nd ECV after a failed ECV?
Yes, all women who request an ECV are offered a 2nd attempt (for those women randomised to the ECV arm only).
What will your approach be to other turning methods eg spinning babies, moxibustion, Webster’s technique?
In the OptiBreech database, we record: 1. Counselling, advice, information and other items (eg. moxa sticks) women have been given antenatally; 2. What women report having used in pregnancy in a follow-up survey 1 month after birth
Will women have to agree not to try them or will they be allowed or even encouraged? In either case the data on what else they try will need to be collected.
Currently, the OptiBreech care pathway does not include specific advice on complementary therapies. We are collecting observational data on their use only. We will neither be requiring women not to try complementary therapies nor encouraging them to do so.
Hope that helps! Keep up the good work!!!
Thank you!
OptiBreech is helping so many women that are coming through our group – I hope you can find a way to make it more widely adopted once the research is completed (but I realise the NHS is slow…)
We are working on that too! Watch this space …
Responses to the online survey
Who participated?
Other: I experienced undetected footling breech presentation and delivered vaginally at home prior to midwife arrival due to rapid labour. Just over 2 months ago.
Q1 – What do you like about this study?
I felt like my only option was elective c-section so this would have been great to support a vaginal breech birth for me
I am interested to know if not attempting an ECV would lead to better outcome. And how good are the outcomes for mum and baby in BVV.
Having options to birth vaginally rather than being told you must have a c section. That there will be specialists in breech aginal delivery
That it could support trusts to support VBB
The encouragement of the use of natural breech birth
The results can influence that women should not be forced into an ECV automatically. Autonomy is so important
Each study arm has an emphasis on vaginal birth; the study will collect good data on the outcomes of VBB attempts in general and this will allow more birthing people to consider a VBB, with or without ECV.
It could provide some insight to the reality of the benefit of ECV rather than a perceived benefit. Any additional information on breech birth will help empower women with their birth choices.
I like that methods other than ecv are being looked at.
Its taking a good look at optimum care for women with a breech presentation, acknowledging that they may want a vaginal birth and this is a perfectly reasonable option.
It is lookind xarefully at the impact of ECV. It is supporting vaginal breech birth
I like that women would be allowed to make an informed choice without being pressurised into what they don’t want, considering there are no further risk factors involved
It looks at the clinical benefits and outcomes of a procedure which is often just assumed, or denied without a real discussion
Providing more data on the benefits of an ECV to allow people to make informed choices
I like the idea that in one group the baby decides- if it stays breech it can be born breech. I like that both groups will get to birth vaginally
I think ECV can seem like ‘an automatic’ thing to do when your baby is breech. I think it is important to look into this into more depth as it never really has been done before. I had an ECV but if I were to have another child who presented breech I would not have one and either wait for baby to turn or go for a vaginal birth (if no contradictions)
I like that you are looking at the various options of breech babies & better outcomes. If it leads to women being able to choose to birth vaginally instead of being coerced into a c-section then I am all for it. We need more education about vaginal breech births in the NHS
It is looking to educate and empower and provide HCPs with a level of experience in delivering breech babies that is severely lacking within the NHS. Looking to inform woman that breech is normal and not in isolation, a reason for concern.
Having an ECV is very stressful, and though risk is low, safety can’t be guaranteed. If there is no additional benefit to having one, it’s potentially an unnecessary and step leading to less successful vaginal births. If safe breech vaginal delivery was normalised, women may be less scared into having an ECV
Simple design
Q2 – Did anything concern or worry you?
No
No.
No
No
no
Not really
No
Not currently.
No. But I know some women worry about ECV. I had one (which didn’t work) so I’m not bothered.
What about thoae who wish to birth at home?
No
No
No
No, I think this is well thought out research
No
That this is purely about whether or not to have an EVC. Also will it lead to yet another thing to coerce women into doing?
There is a lot of coercion within maternity care. No matter the guidelines, assurances or gaslighting that goes into denying or covering it up. I would be concerned as a mother anticipating a breech baby that when I came to labour, a medical team who did not support the trial would be charged with my care. I would be denied my birthplan. That any slowing or deviations from a classic progression and delivery would be blamed on the breech and so start the process of implanting doubt and then coercion of a woman in a vulnerable state of labour towards a section as this is the route that the clinicians feel they have the most control of the outcome.
To encourage more women to participate, they should be able to swap groups if they feel more comfortable having or not having an ECV when the time comes
I supposed if someone was randomised they took ECV and really wanted one they could opt out, or vice versa
Q3 – Was there anything you needed more information about, or felt was unclear in the summary?
Note: Where participants expressed questions, we answered these above.
No
No
No
yes
No
Very clear
Does this include footling breech presentation? As all basic literature I have found suggests c section always offered with these.
How do people get consented to the randomisation
I’d want more information about what OptiBreech is, but appreciate this may confound the research. I suspect the research will take place in hospital, but that hasn’t been made clear.
No
No
No
No, it was all clear
No
If a person has birthed before… are first time persons more likely to be reluctant to participate. Once you have experienced labour and birth are you more likely to elect for a breech? I think I would have been reluctant with my first (head down) as birth was venturing into the unknown but I personally wanted to with my second. Sadly I wasn’t given the option. My trust informed me I was either successful ECV or it had to be a section as there wasn’t anyone who would deliver a breech baby. It wasn’t until much later that I realised that I had been bullied into consenting to an unnecessary procedure and not given any time to make an informed decision.
No, very clear
Perhaps that person giving birth always has a choice about the treatment they pursue
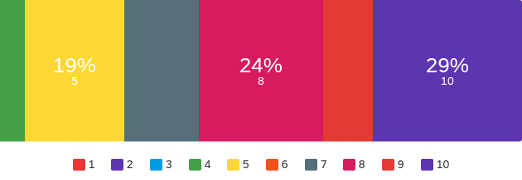
Q4. If we asked 10 women or birthing people who prefer a vaginal birth if they would like to participate in this study, how many of these 10 women do you think will agree to participate?
Minimum: 4
Maximum: 10
Mean: 7.76
Standard deviation: 1.95
Q5. If you were pregnant with a breech baby, would you participate in this study?
All 21/21 women who participated in our survey indicated they would participate in this study.
Q6 – Why do you feel this study will be acceptable, or not?
Yes
I think it’s acceptable, it’s an interesting topic
Acceptable because it gives women choices with their bodies and births which reduces trauma surrounding a lack of control to try birth vaginally
Na
yes
Anything that gives women autonomy is so important, as they have to deal with the consequences of it. You shouldn’t be made to feel that is the only option
Dedicated care for breech presentation to optimise the chances of a successful vaginal birth in both arms.
It may be tricky because VBB can be taboo, and offering ECV is a standard of care. Some women may feel they are not giving themselves the best chance if they don’t attempt an ECV
Some women won’t want to risk having an ECV.
If birthing people have strong feeling ref ECV they may withdraw if allocated to the ‘wrong’ group.
It allows women making informed choice whilst considering research data and risk factors
This is a really vulnerable time in a pregnancy. Women often have ideas about how they are going to give birth, they are often told for weeks/months don’t worry baby has lots of time to turn and then suddenly it’s all systems go for a c section. It should be talked about more throughout with real tangibility of success rates and impacts
Support of the OptiBreech team will mean candidates are more likely to support a randomised study as they will feel well cared for by experts
I’m both groups there is clearly good care and support from a breech team
It looks into the area in more depth and gives women and birthing people more information as a result
Education on babies needs to be bought to the table.
Anything to enable fewer interventions in a healthy pregnancy and labour can only be beneficial.
If I was pregnant for a second time with another breech baby I would definitely participate as I’m no longer concerned about having a breech vaginal delivery following my participation in the Optibreech trial. Had this opportunity been given to me with my recent breech pregnancy, I would have preferred to have a choice as to which group I was allocated as I wanted to try and turn my baby. If safe breech vaginal deliveries were normalised and it was well known that having a breech team meant a safer delivery than all modes of birth, I think I would have been relaxed about whether to have an ECV or not and therefore willing to participate in either group.
Not a very high risk procedure. Painful though
Q7 – Is there anything else you would like us to prioritise for OptiBreech research?
Further expanding OptiBreech sites/upskilling more midwives and HCP so more women and birthing people have a real choice
I would like to learn more about the outcomes of the VBB when attempted with help of an experienced team.
The collection of evidence to support VBB and VBac
Could woman opt in for ECV or no ECV themselves?
Any data on VBB home birth.
Supporting women in any location.
Getting all hospitals to offer real choice to pregnant women
Yes – educating healthcare workers that breech is ‘normal’ – not a disaster waiting to happen.
It would be interesting to know if labour during breech vaginal deliveries is quicker than head down.. I think I read somewhere that it is? With regards to labouring at home and knowing how soon you should go into hospital. Should women labouring with a breech baby be encouraged to attend hospital sooner than head down.
Na
We also asked for permission to include the quotes provided in our report. Thank you to all those who have helped us to shape this research and our on-going projects.