All invited to this participatory research webinar, where we will share findings from our qualitative research and invite you to shape our interpretations!
Sharna, Cianna, their family and their midwife, Anne
In this participatory research webinar, we will share the results of two of the OptiBreech qualitative research projects. We invite all stakeholders (participants, women & birthing people, clinicians, service leaders and policy makers) to reflect on our findings with us and shape the interpretations we will summarise in our papers’ discussions.
Work will be presented by Research Assistants Honor Vincent and Alice Hodder, along with our PPIE Lead, Sian Davies. Abstracts of the two papers are below. If you have contributed to the research (clinicians and research staff), you will receive a copy of our draft paper and an invitation to make comments and/or recommendations for revisions.
If you are a stakeholder, we invite you to share your views in the meeting chat, raise them when we open the meeting for discussion or send them directly to a member of the research team.
For all sites that have expressed an interest in our planned stepped wedge trial of OptiBreech collaborative care: please include your name and hospital in the webinar chat, and we will award one site selection point for every site that participates.
Barriers and facilitators for team implementation of OptiBreech collaborative care
Introduction: Increased rates of caesarean section for breech presentation and lack of training have reduced professional experience and expertise in supporting vaginal breech birth. OptiBreech collaborative care is a care pathway that aims to enable maternal choice and improve training opportunities for maternity professionals, through dedicated clinics and intrapartum support. In feasibility work, barriers and facilitators to team implementation were observed by team members. This study seeks to describe these factors to optimise future implementation of OptiBreech collaborative care.
Methods: Semi-structured interviews were conducted with staff members at OptiBreech trial sites (17 midwives and 4 obstetricians, n=21), via video conferencing software. A Theoretical Domains Framework (TDF) was used to identify factors impacting team implementation. Themes identified in the TDF were refined in reflective discussion and grouped into key facilitators, key barriers, and dynamic factors (which span both barriers and facilitators). The interviews were then coded, analysed and interpreted according to the refined framework.
Results: The key facilitators were broadly categorised within skill development, beliefs about capabilities and social support from the wider multidisciplinary team. Key barrier categories were resources, social obstacles and fears about consequences. Dynamic factor categories were individual responsibility, training and practice.
Conclusions: While some factors affecting implementation were specific to the individuals and cultures of certain trusts, recommendations emerged from analysis that are more broadly applicable across multiple trusts. These should be considered going forward for future trust implementation in the next stage of clinical trials.
The OptiBreech Trial feasibility study: a qualitative inventory of the roles and responsibilities of breech specialist midwives
Background: The safety of vaginal breech birth (VBB) is associated with the skill and experience of professionals in attendance, but minimal training opportunities have led a to a lack of willingness to support these births. OptiBreech collaborative care is a pathway designed to support maternal choice and professional training, through dedicated breech clinics and intrapartum support. In feasibility work for the OptiBreech Trial, these were usually co-ordinated by a key midwife on the team, functioning as a specialist.
Objective: To describe the roles and tasks undertaken by breech specialists in the OptiBreech 1 study (NIHR300582).
Methods: Semi-structured interviews were conducted with OptiBreech team members (17 midwives and 4 obstetricians, n=21), via video conferencing software. Template analysis was used to code, analyse, and interpret data relating to the roles of the midwives delivering breech services. Tasks identified through initial coding were organised into five key themes in a template, following reflective discussion at weekly staff meetings. This template was then applied to all interviews to structure the analysis.
Results: Breech specialists as change agents emerged as important in multiple settings; each fulfilled similar roles to support their teams, whether this role was formally recognised or not. In this study, this role was most commonly described as fulfilled by midwives, but some obstetricians also functioned as specialists. We report an inventory of tasks performed by breech specialist midwives, organised into five themes: Care Planning, Clinical Care, Education and Training, Service Development, and Research.
Conclusions: Breech Specialists perform a consistent set of roles and responsibilities to co-ordinate care throughout the OptiBreech pathway. The inventory has been formally incorporated into the OptiBreech collaborative care intervention. This detailed description can also be used by employers and professional organisations who wish to formalise similar roles to meet consistent standards and improve care.
Read why our collaborators would like to help extend the provision of OptiBreech care by participating in a cluster trial.
As we prepare our funding bid to scale up OptiBreech care around the UK and evaluate it in a stepped wedge cluster trial, we have invited NHS sites to formally express an interest in collaboration. We are pleased to share some of our collaborators and the reasons they are joining this trial.
Walsall Healthcare NHS Trust
Lead: Joselle Wright, Head of Midwifery
“We are a smaller DGH with 3700 births, smaller units often do not get the opportunity to participate in these amazing research studies. This would be a great opportunity for our women.”
Shrewsbury and Telford NHS Trust
Lead: Dr Olusegun Ilesanmi, Consultant Obstetrician
‘Research within our Trust is important as this enables us to ensure we provide up to date evidence based safe care, with Women & their babies at the centre. The Opti Breech Study promotes informing Women about their options and to plan their care with them rather than making decisions about them, as well as improving our expertise, knowledge, and staff development. We look forward to giving Women within our care the opportunity to be part of the Opti Breech Study’
Maidstone and Tunbridge Wells NHS Trust
Lead: Charlotte Gibson, Consultant Midwife
Maidstone & Tunbridge Wells OptiBreech Team-to-be a the RCOG, May 2023
‘This is an exciting opportunity for us to support women’s health research which will positively impact those who provide care, the service we are able to offer and ultimately optimise health and well-being outcomes for those we care for. All with the added and far-reaching benefit of growing and strengthening our clinical research culture and capabilities within our service, community and beyond. It was from women’s and families lived experiences that led us to embark on setting up a Breech Birth Faculty. Our aim is to build the capabilities and confidence within our workforce to support safe and personalised care for those who have a breech baby at term. Collaborating with the Opti Breech Trial will be fundamental in achieving this aspiration.‘
West Hertfordshire Teaching Hospitals NHS Trust
Lead: Claire Church, Consultant Midwife
“We would like to get involved in Optibreech so that we can offer a comprehensive, standardised service to our women and birthing people with breech babies which ensures that they are all counselled in the same way and given informed choice regarding their options. We also want to provide our staff with the skills and competencies to support our women and birthing people with their choices and feel confident in doing so”. – (Clare Church. Consultant Midwife)
North Tees and Hartlepool NHS Foundation Trust
Lead: Kirsty Farrington, Sharon Gowans and Julie Woollaston – Research Midwives
‘We are really excited to be involved in this research! It is a great opportunity to not only work towards delivering evidence-based care for women but also to develop skills and build confidence within the whole maternity workforce.’
NHS Lothian, Royal Infirmary of Edinburgh
Leads: Rosemary Townsend and Andrew Brown, Consultant Obstetricians
Wirral University Teaching Hospital
Lead: Consultant Midwife Angela Kerrigan
It will be fantastic to be involved in the Optibreech trial as it will offer additional skills to our staff to enable us to provide an enhanced service to women who present with breech presentation at Term through the Optibreech collaborative care pathway. This is really a exciting trial to be involved in that has the potential to positively influence the care of women with babies presenting breech at Term.
Wrightington, Wigan and Leigh Teaching Hospitals NHS Foundation Trust
These principles underpin the new JRCALC guidance on breech birth, due to be published next month. Ambulance clinicians, keep your eyes out 👀 #Breech#JRCALChttps://t.co/jCkvpcbs9j
Expressions of interest are invited for sites to collaborate on an HTA funding bid for a stepped wedge cluster trial of OptiBreech care.
We are aiming to submit a funding proposal in August 2023 and if successful, plan to begin work on the trial in summer 2024. We hope to include sites from Scotland, Wales, Northern Ireland and England, with a preference for sites outside of London that benefit from participation in research less frequently.
We expect to part-fund a developmental breech specialist midwife post. This is a highly sought-after position that is likely to attract external applicants and contribute to staff retention.
Participating sites get unlimited free in-person and on-line training that has been fully evaluated in NHS settings,* support with implementation and involvement in OptiBreech community of practice. * This is the same training offered through the RCOG.
Women would retain choice of ECV/no-ECV and mode of birth. We expect a modest increase in planned vaginal breech births in most settings.
Kate Walker, Clinical Professor of Obstetrics, University of Nottingham
Debra Bick, Professor of Clinical Trials in Maternal Health, Warwick Clinical Trials Unit
Kate Stringer, Consultant Midwife and Implementation Lead, Surrey and Sussex Hospitals
Rosemary Townsend, Senior Clinical Fellow in Obstetrics, University of Edinburgh
Andrew Brown, Consultant Obstetrician and Skills Training Lead, NHS Lothian
Amy Meadowcroft, Breech Specialist Midwife and NIHR PCAF, Oldham
Siân Davies, Perinatal Psychologist and PPIE Lead
What is OptiBreech collaborative care?
OptiBreech care is a new care pathway for delivering standard care to women and birthing people pregnant with a breech-presenting baby at term. This population is defined as: breech presentation at birth, or at any scan from 35+0 weeks or where a successful external cephalic version (ECV) has been performed.
Phase 2 @optibreech is looking for new sites! See EOI for more info- https://t.co/8n9uZRMSeL We are keen to engage sites with varying demographic and size across 🇬🇧 Funding/training/implementation to set up Breech Clinic and services. DM for 1:1 or more info. Happy to discuss
The service is provided through a dedicated clinic, co-ordinated by a breech specialist midwife, working collaboratively with a breech lead obstetrician. All management options are offered – external cephalic version, vaginal breech birth and elective caesarean birth. ECV attempts are provided by clinic staff in a same-day service where required. Intrapartum care for vaginal breech births follows the OptiBreech physiological breech birth guideline, developed by the OptiBreech Collaborative. The breech lead midwife and obstetrician lead on training throughout the service, including mandatory updates and simulations. The specialist midwife also co-ordinates a continuity of care service, so that whenever possible planned breech births are attended by a member of the team with full OptiBreech training and experience managing complications. Members of the team are also part of an extended OptiBreech community of practice, which provides regular practice updates and opportunities for reflection as they develop competence and expertise.
How does this differ from standard care?
This is a new way of organising care and training for breech presentation at term. Current standard care is characterised by a lack of standardisation and adherence to national guidelines from the RCOG(1) and NICE(2). OptiBreech care promotes standardisation for optimal outcomes. The vaginal breech birth training that is provided is the same training offered on the RCOG Labour Ward Management course, RCOG Vaginal Breech Birth study days and Royal Society of Medicine Maternity and Newborn Forum, which led by clinical members of the research team.
These principles underpin the new JRCALC guidance on breech birth, due to be published next month. Ambulance clinicians, keep your eyes out 👀 #Breech#JRCALChttps://t.co/jCkvpcbs9j
Why do we think a cluster trial is appropriate now?
There is strong evidence current standard care pathways do not provide consistent access to all options national guidelines recommend,(3,4) nor do they provide adequate training opportunities for younger obstetricians and midwives.
OptiBreech collaborative care is a pathway developed with significant input from service users and clinicians. It is highly acceptable to women and birthing people, regardless of their care choices or ultimate mode of birth.(5)
Feasibility work has included two NHS training evaluations,(6,7) an observational implementation evaluation and a pilot trial. All three have demonstrated better outcomes compared to standard care for vaginal breech births. For example, the neonatal serious adverse outcome rate for women planning a vaginal birth has been less than 1%, compared to 5% in the Term Breech Trial,(8) and 7% for actual vaginal births in standard care births included in our training evaluation.(7)
The pilot trial demonstrated that women have access to all three guideline-recommended options within the OptiBreech care pathway, but not within standard care (see below).(9)
Pilot trial results: More women planned a VBB when randomised to OptiBreech Care (23.5% vs 0, p = .003, 95% CI =.093,.378). Women randomised to OptiBreech care had: lower rates of cephalic presentation at birth (38.2% vs 54.5%), higher rates of vaginal birth (32.4% vs 24.2%), lower rates of in-labour caesarean birth (20.6% vs 36.4%), lower rates of neonatal intensive care (5.9% vs 9.1%), and lower rates of severe neonatal morbidity (2.9% vs 9.1%). Within the entire cohort, breech presentation on admission to labour/birth (n=44), compared to cephalic presentation (n=38), was associated with: lower levels of neonatal admission (2.3% versus 10.5%), lower levels of severe neonatal morbidity (2.3% vs 7.9%), fewer maternal admissions to HDU (4.5% vs 7.9%) and less severe maternal morbidity (13.6% vs 21.1%). Outcomes for non-British and non-white women were also better than participants from white British backgrounds, which reassures us this service is accessible to minoritised participants. Randomisation was stopped in June 2022 on the advice of the steering committee, at 68 women randomised rather than the planned 104. It was clear 1:1 randomisation would not enable us to compare outcomes for VBB because women were not choosing to plan a VBB within standard care.
We know that the model enables access to a guideline-recommended care option (VBB), but we do not know how this will affect outcomes. A definitive trial that is powered on serious adverse neonatal outcomes is urgently needed and could lead to the implementation of OptiBreech collaborative care across the NHS.
What outcomes do we expect to improve with OptiBreech care?
Based on the results of our feasibility work and the available literature, we think that the rate of serious adverse neonatal outcomes (including death, HIE, admission to the neonatal unit >4 days) is about 4.5% for the entire cohort of term breech babies within standard care, as defined above. We think we can reduce this by about 40%, to 2.7%. This is the primary outcome we are seeking to improve.
We also think that OptiBreech care will be more cost-effective and reduce the rate of emergency caesarean birth.
How do we think OptiBreech care will do this?
We expect up to 1-2 women per month at each centre to plan a vaginal breech birth, with no increase in adverse outcomes for these babies. (Note: This is an estimate of what might happen when services are delivered in this way, but there is no target VBB recruitment rate. Women’s choices remain the same.) Your site will implement the new care pathway for women booked at your service but will not be promoted as an OptiBreech referral site.
Based on available evidence and our feasibility work, we expect a reduction of 0.9% of serious neonatal outcomes will come from increasing skill levels throughout the service, learning from these planned events, and improving mandatory skills training to bring it in line with the most current evidence. We think this will help prevent adverse outcomes in unanticipated vaginal breech births.
In multiple audits and our pilot trial, we have also observed that within this model of care more women choose an elective caesarean birth, and the emergency caesarean birth rate declines. This will result in 0.9% additional improvement in neonatal, maternal and economic outcomes.
How will we evaluate this?
We will evaluate this in a stepped wedge cluster trial, including twenty sites over three years. If your site is chosen to participate, you will implement the care pathway at a point during the three years determined through randomisation. Our research team will analyse outcomes for women receiving care at the sites prior to and after randomisation.
What support would participating sites receive?
If you are one of twenty sites chosen for this trial, your hospital will receive unlimited free physiological breech training. This training is currently provided through the RCOG at a cost of over £360/person. We will train any members of your team you would like to receive full training. We will also train your skills trainers to deliver updates through standard mandatory training activities and periodic simulations.
At this point, we hope to be able to fund one half day per week of a Band 7 breech specialist midwife developmental post. This person will be a current Band 6 ready to step up to greater leadership within the service. They would need to be in post for between one to three years, with associated funding between £12,126 and £36,379, depending on your site’s starting point in the trial. They would be supported by senior members of your team to develop into a specialist. Your breech specialist midwife will also collect the data for the study, and the time for this will also be funded through the CRN; this is likely to be approximately 0.1 WTE, depending on the size of your service. This is a desirable post for the right person, which we anticipate will contribute to staff satisfaction and retention, in addition to developing your breech service.
We would provide you with a comprehensive job description, guideline and training resources, operational during the time your site is ‘live’ on the trial. This guideline has been developed by the OptiBreech Collaborative, clinicians who have led the first stages of feasibility work for this trial.
We would provide you with support during the implementation period from an experienced member of our team who has successfully implemented the service we are testing. And we would provide support through our community of practice activities for all members of your team who wish to participate. These include regular practice updates, case reviews and opportunities for reflective supervision with clinicians experienced in supporting physiological breech births. As many new sites will have limited recent experience supporting planned vaginal breech births, this will be re-introduced in a controlled and supported way.
Why else should you consider participating?
If this trial has a positive result, the OptiBreech collaborative care pathway will likely become the standard of care, and you will have already implemented it. If the trial does not demonstrate an improvement in outcomes, your team would still have acquired significant experience in the management of vaginal breech births, which may still bring beneficial skills and knowledge into your service.
Where can I read more about the research supporting OptiBreech care?
Please complete this form with your name and contact information. We will contact you with more information about requirements for site selection.
References
1. Impey L, Murphy D, Griffiths M, Penna L, on behalf of the Royal College of Obstetricians and Gynaecologists. Management of Breech Presentation. BJOG [Internet]. 2017 Jun;124(7):e151–77. Available from: http://doi.wiley.com/10.1111/1471-0528.14465
4. Roy R, Gray C, Prempeh-Bonsu CA, Walker S. What are women’s experiences of seeking to plan a vaginal breech birth? A systematic review and qualitative meta-synthesis [version 1; peer review: awaiting peer review]. NIHR Open Research 2023 3:4 [Internet]. 2023 Jan 20 [cited 2023 Jan 21];3:4. Available from: https://openresearch.nihr.ac.uk/articles/3-4
6. Walker S, Reading C, Siverwood-Cope O, Cochrane V. Physiological breech birth: Evaluation of a training programme for birth professionals. Pract Midwife. 2017;20(2):25–8.
8. Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. The Lancet [Internet]. 2000/10/29. 2000 Oct 21;356(9239):1375–83. Available from: http://www.ncbi.nlm.nih.gov/pubmed/11052579
9. Walker S, Spillane E, Stringer K, Trepte L, Davies SM, Bresson J, et al. OptiBreech collaborative care versus standard care for women with a breech-presenting fetus at term: a pilot parallel group randomised trial to evaluate the feasibility of a substantive trial nested within a cohort. In peer review. 2023;
Stakeholder Engagement
Funding for the Breech Specialist Midwife post at Band 7
The activities performed in a breech clinic are not new. ECV, VBB and caesarean birth are all guideline-recommended choices and RCOG-recommended auditable services. Offering them through a dedicated clinic with a small teams with a high level of skill and experience is new. The change management required to shift these tasks into a dedicated clinic, develop the skills to run the clinic and manage the service so that staff who need training are able to rotate through the clinic – this is the ‘new’ thing that requires extra organisational time and incentives. But once in place, it helps all of the basic services run more efficiently, at a higher standard.
Few opportunities for progression – Discussions with midwifery managers and staff outside of the southeast of England indicated there are few opportunities for midwives to progress in their careers to a senior midwife post. For this reason, we will require the appointment to be at least a beginning Band 7. We want the post and the project to offer greater opportunities to health boards and hospitals that benefit from participation in research less frequently.
Not enough research staff – The breech specialist midwife will be seconded to the research team for at least 10% FTE (half a day a week). The funding will this will come from the Clinical Research Network (CRN) pots that fund all research midwives and nurses. Collecting service data also contributes to the breech specialist’s growing expertise. By the end of the project, they will have additional transferrable skills to remain active in clinical research, either through further work as a research midwife or by pursuing a clinical academic role. It also offers the specialist increased flexibility in their working patterns. Sometimes, a clinic day is not full of breech-presenting babies; data can be collected. Sometimes, there is a late diagnosis of breech presentation requiring urgent counselling; or a birth occurs overnight before a research shift; data collection can easily be rescheduled.
Will anyone be willing to take on the role? Managers worried that the post would require someone to take on a lot of responsibility and that their staff are often very junior due to staffing shortages. They often expressed worry that they might not find someone willing to take up the post. However, often in the same conversation, someone was simultaneously offering to fill the post or identifying someone who would be very keen to ‘own’ the project locally. Our experience is also that experienced junior staff often ‘grow’ in this position, as it gives them an opportunity to expand their skills and autonomy with support. However, due to this worry, we will work with sites who express an interest to ensure they have identified someone who is willing and able to take up the position in advance of confirming them as a collaborator on the funding bid.
Most obstetric staff who expressed an interest were very keen to participate but worries that they were not seeing sufficient numbers of women planning a vaginal breech birth to make it worthwhile.
There is no VBB target. We have reassured sites that this study is NOT about promoting vaginal breech birth, and there is no minimum target of VBB numbers to achieve. If no one plans a VBB, and one-month follow-up surveys indicate that they felt well-informed and supported, with all choices available, there is no problem! If on the other hand, follow-up surveys indicated women are meeting resistance when they attempt to plan a VBB, we would work with sites to address this.
“There are many barriers within our service.” Multiple obstetricians who were otherwise keen to support women’s choice to plan a VBB described the same barriers within their service:
Not all women eligible were referred for an ECV attempt. Many were just encouraged to plan a caesarean section. (This aligns with available systematic review evidence, our interview data and our PPI feedback.)
When women chose to plan a VBB after a failed ECV, they often wanted to return to talk about it a bit more. But they returned to their named consultant’s clinic and were discouraged, so many abandoned their hope to plan a VBB. (This aligns with available systematic review evidence, our interview data and our PPI feedback.)
Some women felt confident to plan a VBB with appropriate counselling, but when they arrived in labour, it was very clear that the clinical team on duty were not supportive. Often, they would find any excuse to recommend an emergency caesarean early in labour, eg. suspecting a ‘footling breech’ at 2 cm when previous scans have indicated an engaged pelvis. The few women who continued to plan a VBB often ended up feeling very let-down and disappointed with the service. (This aligns with available systematic review evidence, our interview data and our PPI feedback.)
Because of this, obstetric staff often felt frustrated that, although they wanted to participate, it might not be possible in their setting.
This is the problem in almost ALL settings. You are not alone! The standard care pathway is not working in most settings for precisely these reasons. That is why our proposed intervention is a care pathway intervention. Even if we have improved the safety of VBB, if there is no way for women to benefit from this, and no way for staff to learn from it, nothing will change. This is the problem our ‘intervention’ (a dedicated clinic and service, co-ordinated by a breech specialist midwife) is designed to improve. Once you ensure that women receive consistent counselling and continuity of care, you can begin to benefit from improved training and cultural change.
New publication: Women’s experiences of seeking to plan a vaginal breech birth: a systematic review and qualitative meta-synthesis.
The extended OptiBreech team is pleased to announce a new publication.
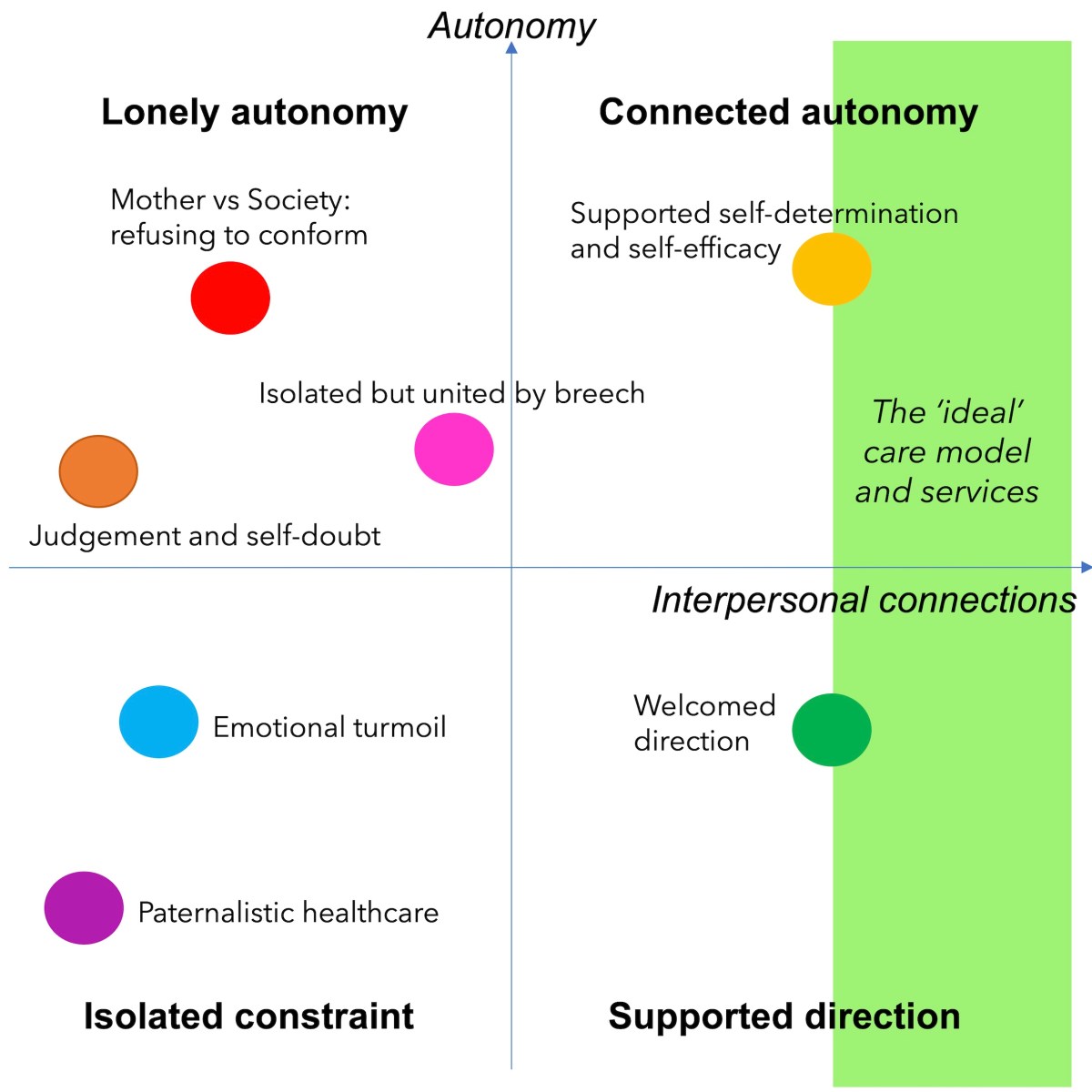
Ceclia Gray and Ritika Roy (joint first authors) lead a systematic review and qualitative meta-synthesis of women’s experiences of seeking to plan a vaginal breech birth. Gray and Roy are King’s College London medical students who were funded to undertake this work by King’s Undergraduate Research Fellowships.
Women seeking to plan a VBB feel vulnerable and wish to connect with capable and confident healthcare providers. To meet their needs, services should be designed so that they can connect with clinicians who are willing and able to support their autonomy. Services should also seek to limit their exposure to disrespectful and judgemental interactions with healthcare providers.
Gray and Roy were joined by service user co-researcher Charlene Akyiaa Prempeh-Bonsu, who planned a vaginal breech birth in the NHS herself within the past five years. Prempeh-Bonsu contributed to data analysis with support and reflective discussions. She helped to ensure the work reflected the needs and interests of the population being described.
What has your experience been? Have you planned (or tried to plan) a vaginal breech birth within the UK NHS? We invite you to leave a comment below. Please let us know if you gave birth within an OptiBreech site, or not.
An initial objective of this research is to develop a core outcome set for effectiveness trials of vaginal breech birth (COMET). Establishing a core outcome set enables the results of trials to be combined and compared in meta-analysis and gives us a way to judge the effectiveness of interventions across settings.
If it does not prove feasible to conduct a randomised trial, a different design may work better. For example, a large prospective observational study, using the same core outcome criteria. While many sites within the UK are implementing physiological breech birth, many successful early adopters are outside of the UK. Collaborating with them will enable each of us to demonstrate local results, and to identify the incidence of rarer outcomes such as perinatal morbidity and mortality (death or serious illness around the time of birth).
Therefore I am proceeding with both potential projects in mind, so that the work has a flexible back-up plan for providing the answers that women and health care professionals want about physiological breech birth. I have applied for a smaller grant, which would fund the outcomes consensus project and creation of an on-line database, to which collaborators anywhere in the world could contribute once local approvals are obtained. If both applications are successful, the international prospective observational study would provide evidence of the generalisability of any results we see within the UK study.
International collaborators who have agreed to lead data collection in their countries are:
Germany — Dr Anke Reitter, Chief Obstetrician, Krankenhaus Sachsenhausen, Frankfurt
Australia — Dr Andrew Bisits, Director of Obstetrics, Royal Hospital for Women, Sydney
Denmark — Dr Kamilla Gerhard-Nielsen, Obstetrician, Syghus Sønderjylland, Aabenraa
Netherlands — Dr Floortje Vlemmix, Amsterdam Universitair Medische Centra; and Dr Leonie van Rheenan-Flach, OLVG West, Amsterdam
Sweden — Dr Julia Savchenko, Obstetrician, Södersjukhuset, Stockholm
Canada — Jane Wines, Midwifery Lecturer, University of British Columbia
Ethiopia — Kidist Eshetu Berhahu, Hawassa College of Health Science, Ethiopia; and Shimeles Tsegaya Tessema, Dilla University
Hungary — Dr Zoltan Kovacs, Obstetrician, Robert Hospital, Budapest
Brazil — Professor Melania Amorim, Senior Researcher & Obstetrician, Instituto Paraibano de Pesquisa Professor Joaquim Amorim Neto (IPESQ) and Dr Priscila Ribeiro Huguet, San Paolo
Belgium — Dr Caroline Daelemans and Dr Sara Derisbourg, Erasme Hospital, Brussels
India — Dr Evita Fernandez and Indie Kaur, Fernandez Hospital Foundation, Hyderabad
United States — Dr Emiliano Chavira, St Francis Medical Centre, and Dr Annette Fineberg, Sutter Davis Medical Centre, California, USA
Spain — Carmen Medina Mallen, Hospital de Sant Pau, Barcelona
If you are potentially interested in collaborating in this project, please contact me via the form below.