Dear Shawn
Trust all is well at your end
Shawn as we are not doing optibreech trial do we need to change anything at our end especially with regards to legality etc.
some queries which have cropped up here
What is the frequency of training?
Is this MDT training?
Who runs the training?
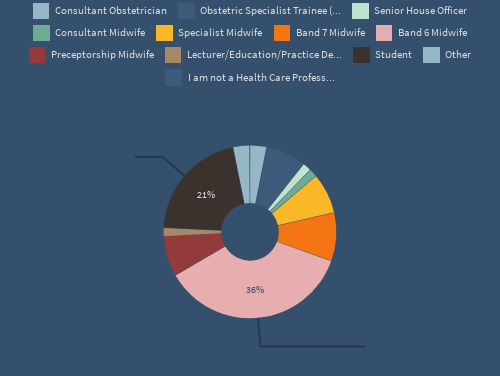
Optibreech trained staff – numbers and skill mix?
What is the compliance for completion of vaginal breech birth training offered?
Is there a lead for the Optibreech trial – may be helpful to meet with them?
Also otherwise any legal changes etc ….
The OptiBreech pilot trial and feasibility study ended on 31 January 2024. The team made four applications for further funding, but unfortunately funding for a substantive trial was not gained. Without further funding, we will not know the effects of full implementation of the OptiBreech Collaborative Care pathway as the standard care pathway for breech care in the UK.
The evidence from the pilot work indicates better outcomes than any prospective study previously done, especially in the UK. This may change with greater numbers, but without further research, we will never know. Our early economic modelling suggests that the care pathway is likely to be cost effective. Again, without a substantive trial, we will never know.
Many of the sites that participated in the pilot and feasibility work have continued to offer the OptiBreech Collaborative Care pathway to women pregnant with a breech-presenting baby late in pregnancy. When they have had less than ideal outcomes, as is inevitable, those offering this model of care have come under increased pressure to justify offering a service that has not been demonstrated in a full RCT to improve outcomes, compared to standard care.
This is therefore a good time to explain exactly what OptiBreech Collaborative Care is, how it differs from standard care, and if the lack of RCT-level evidence should be a barrier to offering this model of care to women.
What is OptiBreech Collaborative Care?
First of all, OptiBreech Collaborative Care is a care bundle, or care pathway, rather than something entirely new and different from ‘standard care.’ The model organises the elements of care women need to make an informed choice about their planned mode of birth for a breech baby, and to optimise the chances that the outcomes will be good if a woman chooses to plan a vaginal breech birth.
The ways the pathway differs from standard care are outlined below.
A dedicated clinic, co-ordinated by a breech specialist midwife, in collaboration with an obstetric lead for breech
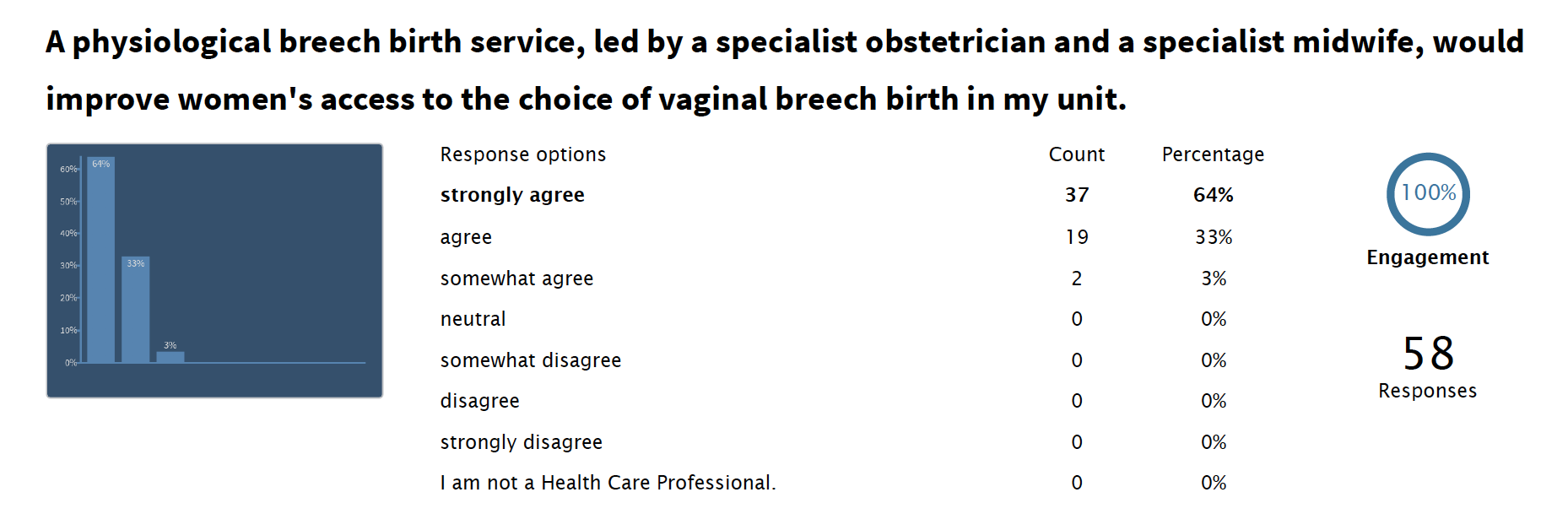
UK national guidelines state that women should be supported to make an informed choice about their planned mode of birth for a breech-presenting baby at term. All of the available qualitative evidence indicates that currently in the UK, the majority of women who might wish to plan a vaginal breech birth do not feel that choice is accessible to them and/or they do not feel supported when they make that request.
Qualitative evidence from both women and clinicians contributing to OptiBreech feasibility work confirmed the lack of accessibility of this care option, which national guidelines state that women should be offered. The OptiBreech pilot trial was stopped early because at an interim analysis, there was ALREADY a statistically significant difference in the number of women planning a vaginal breech births under OptiBreech Care compared to standard care, in which none planned a VBB.
Therefore, there is already RCT evidence that the availability of this option, which national guidelines say women should have access to, is improved by providing an OptiBreech clinic within this model. Given that the available economic modelling suggests supporting the option of a safe-as-possible VBB, and the only available RCT demonstrates a significant difference within even pilot-level data in the availability/acceptitibility of this choice, there does not appear to be a pressing need to justify providing care within a dedicated clinic.
Clear definitions of competent, proficient and specialised in vaginal breech birth
What women who wish to plan a VBB say they need from a breech birth service is to know that it is very likely that someone with skill and experience will attend their birth. This is a completely reasonable request, given that the RCOG guideline states that, “with skilled and experienced attendants, planned VBB is likely to be nearly as safe as planned cephalic birth.”
I have been writing about the problematic ambiguity in this statement since it was published. My PhD was dedicated to defining ‘skill and experience’ and how one acquires these within contemporary maternity care. And OptiBreech was/is about finding out how ‘near’ is ‘near.’
Having definitions of proficiency helps enable women to make an informed decision about the support they can expect to receive around the time of birth. This is a discussion that should occur prior to, and during, every birth. If on the day of labour, the only staff available have minimal training, experience and confidence, the birthing person should be informed transparently and supported in their decision to carry on or divert to an early labour caesarean birth.
During the OptiBreech pilot and feasibility work, we provided teams with a proficiency portfolio document to record their experience level, for their own protection and learning, and to accurately inform women. But it was never a requirement. Every clinician has a responsibility to maintain their own records, as it always has been. If Advanced Practice becomes regulated, this is a model for how this might look for breech practitioners at the moment.
All women should have and should be informed that having their birth attended by a skilled and experienced practitioner does not guarantee a good outcome. But it is the only thing ever associated with the improved likelihood of a good outcome.
A plan for getting the right people in the right place at the right time … and a plan for when this is not possible
The most common way that women are discouraged from planning a VBB when they would otherwise like to consider it, is they are told that the staff at this hospital do not have enough experience / a dedicated team / a specialist. And that is the end of the discussion.
There is not a single hospital on the planet where every member of staff feels completely comfortable and competent to support a vaginal breech birth. None. If you try to tell me yours does, I will tell you to go back, speak with each obstetrician privately, and ask them to tell you how they really feel. People always feel pressure to conform, either conform to discouraging the option of VBB so nobody has to do it, or conform to the illusion that anyone can do it.
The reality is, INDIVIDUAL PEOPLE have skills and experience, INSTITUTIONS have people. No institution has a uniform level of skill and experience throughout its maternity staff to support a VBB at the highest level. In institutions that support VBB regularly, INDIVIDUAL PEOPLE may have a high level of skills and additional synergistic experience working with other members of their team, which again improves the safety of VBB.
The only way to increase the chances that someone with skill and experience will be at the birth is to make a plan for it. OptiBreech teams have never had a minimum required number of trained or proficient members. If there are fewer trained practitioners, the chances that one will be able to attend may be lower. If there are more, they may be more likely to ensure an experienced attendants.
But I cannot emphasise enough that many women are grateful if JUST ONE midwife or obstetrician is willing to work flexibly to attend their birth if they can. Requiring staff to have a minimum level of experience in order to ‘allow’ women to plan a vaginal breech birth is not ethical.
What is the frequency of training?
Guidance for what clinicians should do to acquire competence and maintain proficiency is available in previous consensus-based research. In our feasibility work, staff were required to have completed the OptiBreech training, which had previously been evaluated in NHS settings. And they were required to inform women of their experience levels. And the outcomes were very good.
Requiring a further frequency of training in order to ‘allow’ a woman to attempt a vaginal breech birth introduces an obstacle to informed decision-making without any evidence that it will improve outcomes.
Is this MDT training?
The evidence of how we evaluated the training package and with what professionals is readily available. All training, and the research, were multi-disciplinary. National guidance is that Trust internal mandatory training should be multi-disciplinary, and to our knowledge, this is what current OptiBreech sites are doing.
Who runs the training?
In the OptiBreech feasibility study, training was provided by Breech Birth Network, CIC, as this was the only physiological breech birth training that had previously been evaluated in NHS settings. Since the end of the study, sites run their own internal mandatory training and pay to send their staff to the evaluated, full-day study day when they feel it helpful to train new team members. Many breech specialists lead breech training within their own settings, for both midwives and doctors.
Optibreech trained staff – numbers and skill mix?
I am not sure what this question is aimed at. This answer varies for each Trust and for each woman. It varied for each Trust in our pilot and feasibility work.
Again, requiring a certain number of trained staff before women are ‘allowed’ to plan a vaginal breech birth will restrict both women’s informed choices and the ability of any Trust to begin to develop a team. In most sites, building a team began with one person willing to be on-call, until others developed experience and confidence. This strategy resulting in better than standard outcomes.
What is the compliance for completion of vaginal breech birth training offered?
Again, what is this question aimed at? Who is requiring compliance, to what standard, and due to what evidence?
If a clinician says they have completed an evaluated study day in physiological breech birth and they have not, that would be a violation of professional standards. Prior to OptiBreech, there were no proficiency standards, and we have added guidance.
But – to repeat – requiring additional compliance standards will create a barrier to women accessing care from clinicians willing to support their informed choice. With no evidence that requiring some form of ‘compliance’ will improve outcomes.
The only available evidence (from the OptiBreech feasibility and pilot studies) indicates that providing guideline standards and an evaluated physiological breech birth training day for core staff, who then disseminate it to others through mandatory training and skills drills, so far results in an adverse outcome rate that was 1/10th that in the Term Breech Trial (0.5% vs 5.0%).
Is there a lead for the Optibreech trial – may be helpful to meet with them?
Dr Shawn Walker (that’s me) is the lead for the OptiBreech pilot and feasibility trial, which ended on 31 January 2025.