All invited to this participatory research webinar, where we will share findings from our qualitative research and invite you to shape our interpretations!
Sharna, Cianna, their family and their midwife, Anne
In this participatory research webinar, we will share the results of two of the OptiBreech qualitative research projects. We invite all stakeholders (participants, women & birthing people, clinicians, service leaders and policy makers) to reflect on our findings with us and shape the interpretations we will summarise in our papers’ discussions.
Work will be presented by Research Assistants Honor Vincent and Alice Hodder, along with our PPIE Lead, Sian Davies. Abstracts of the two papers are below. If you have contributed to the research (clinicians and research staff), you will receive a copy of our draft paper and an invitation to make comments and/or recommendations for revisions.
If you are a stakeholder, we invite you to share your views in the meeting chat, raise them when we open the meeting for discussion or send them directly to a member of the research team.
For all sites that have expressed an interest in our planned stepped wedge trial of OptiBreech collaborative care: please include your name and hospital in the webinar chat, and we will award one site selection point for every site that participates.
Barriers and facilitators for team implementation of OptiBreech collaborative care
Introduction: Increased rates of caesarean section for breech presentation and lack of training have reduced professional experience and expertise in supporting vaginal breech birth. OptiBreech collaborative care is a care pathway that aims to enable maternal choice and improve training opportunities for maternity professionals, through dedicated clinics and intrapartum support. In feasibility work, barriers and facilitators to team implementation were observed by team members. This study seeks to describe these factors to optimise future implementation of OptiBreech collaborative care.
Methods: Semi-structured interviews were conducted with staff members at OptiBreech trial sites (17 midwives and 4 obstetricians, n=21), via video conferencing software. A Theoretical Domains Framework (TDF) was used to identify factors impacting team implementation. Themes identified in the TDF were refined in reflective discussion and grouped into key facilitators, key barriers, and dynamic factors (which span both barriers and facilitators). The interviews were then coded, analysed and interpreted according to the refined framework.
Results: The key facilitators were broadly categorised within skill development, beliefs about capabilities and social support from the wider multidisciplinary team. Key barrier categories were resources, social obstacles and fears about consequences. Dynamic factor categories were individual responsibility, training and practice.
Conclusions: While some factors affecting implementation were specific to the individuals and cultures of certain trusts, recommendations emerged from analysis that are more broadly applicable across multiple trusts. These should be considered going forward for future trust implementation in the next stage of clinical trials.
The OptiBreech Trial feasibility study: a qualitative inventory of the roles and responsibilities of breech specialist midwives
Background: The safety of vaginal breech birth (VBB) is associated with the skill and experience of professionals in attendance, but minimal training opportunities have led a to a lack of willingness to support these births. OptiBreech collaborative care is a pathway designed to support maternal choice and professional training, through dedicated breech clinics and intrapartum support. In feasibility work for the OptiBreech Trial, these were usually co-ordinated by a key midwife on the team, functioning as a specialist.
Objective: To describe the roles and tasks undertaken by breech specialists in the OptiBreech 1 study (NIHR300582).
Methods: Semi-structured interviews were conducted with OptiBreech team members (17 midwives and 4 obstetricians, n=21), via video conferencing software. Template analysis was used to code, analyse, and interpret data relating to the roles of the midwives delivering breech services. Tasks identified through initial coding were organised into five key themes in a template, following reflective discussion at weekly staff meetings. This template was then applied to all interviews to structure the analysis.
Results: Breech specialists as change agents emerged as important in multiple settings; each fulfilled similar roles to support their teams, whether this role was formally recognised or not. In this study, this role was most commonly described as fulfilled by midwives, but some obstetricians also functioned as specialists. We report an inventory of tasks performed by breech specialist midwives, organised into five themes: Care Planning, Clinical Care, Education and Training, Service Development, and Research.
Conclusions: Breech Specialists perform a consistent set of roles and responsibilities to co-ordinate care throughout the OptiBreech pathway. The inventory has been formally incorporated into the OptiBreech collaborative care intervention. This detailed description can also be used by employers and professional organisations who wish to formalise similar roles to meet consistent standards and improve care.
We discuss potential complications of vaginal breech birth openly, honestly and without sensationalising. 30/8/23 5PM London Webinar. Breech Birth Network welcomes guest host, David Coggin-Carr. David will provide an evidence- and experience-based update on testicular complications of vaginal breech birth.
David Coggin-Carr is a UK+US dual-certified obstetrician, Maternal-Fetal Medicine subspecialist and early career physician-scientist at the University of Vermont (UVM). He practices full-spectrum MFM in Vermont and upstate New York and additionally serve as Associate Medical Director of the Birthing Center and Associate Director of Quality for Obstetrics at UVM Medical Center. In recent years he has developed a strong interest in physiological breech birth in response to the local community’s desire for greater autonomy around their birth choices amidst a near-total lack of trained/experienced providers in the region. Accordingly, he now regularly provides consultations and intrapartum support for planned vaginal breech birth.
Image: Book of Traceable Heraldic Art
All births have the potential for injury, whether this be facial markings from forceps delivery or lacerations from a caesarean birth. Vaginal breech birth has its own variations. This webinar will explore how vaginal breech birth affects neonatal genitals, both normal variations in appearance from being born bottom-first, to potential injuries.
There should be no requirement to report genital injury as a separate category in ALL effectiveness studies of breech birth at term, although it may be reported in some. It should not be included in the Breech-COS composite measure of severe morbidity.
or
The incidence of significant genital injury, defined as one that is likely to have long-term, life-altering consequences, should be reported as a separate category in ALL effectiveness studies of breech birth at term. Significant genital injury should be included in the Breech-COS composite measure of severe neonatal morbidity associated with vaginal breech birth.
For all sites that have expressed an interest in our planned stepped wedge trial of OptiBreech collaborative care: please include your name and hospital in the chat, and we will award one site selection point for every site that participates.
The @OptiBreech team are looking to collaborate with service users who can help us share results with your communities
We have talked about the importance of inclusive research and ensuring the design of studies and trials are shaped by all voices recently. It is also important to consider the dissemination of results and ensuring we reach as many different groups as possible.
Currently, for 39% of OptiBreech participants, English is not their first language. We have a significant number of participants reporting Arabic, Polish, Portuguese, Romanian, Somali, Spanish, Tamil, and Urdu as their first language, with 13% of our participants indicating they need a translator. Additionally, 10% of OptiBreech participants are aged 25 and under.
We therefore would like to reach out to members of our involvement group and previous participants, to form an OptiBreech Results Group. We want to collaborate on developing a strategy to reach as many under-represented communities as we can who may not access our news and events through website updates or traditional media.
This may include making short, self-shot videos helping to communicate the results of our research in your own words and language, especially those results that YOU feel your community will find important. We welcome your ideas on how best to identify the most appropriate outlets to reach as many demographics as we can. You will be reimbursed for any activities with a Love2Shop voucher, in line with the NIHR’s recommended payment rates (approximately £25/hour).
We believe it is important to share data and evidence so that members of the public are aware of their options. We want everyone to have the information to be able to advocate for improved care for themselves individually or alongside their local Maternity Voices Partnership organisation.
Siân Davies, Participant & Public Involvement and Engagement (PPIE) lead.
To express an interest in helping us to disseminate the results of our research with your local community, please complete this form:
Nimisha Johnstone, @OptiBreech PPIE lead, shares women’s views of why it’s important we help babies to start breathing with the cord intact when needed. @NIHRinvolvement
In autumn/winter 2022, the OptiBreech research team spent time developing a research proposal for a study to investigate the implementation of bedside resuscitation for breech babies who require breathing assistance at birth. In my role as a PPI leader with the OptiBreech trial, I sought input from breech presenting mothers and birth workers through small group interviews.
I am the mother of a baby who presented breech at the end of pregnancy. I planned a vaginal breech birth and agreed to allow my birth data to contribute to the OptiBreech study in 2021. Since then, I have become involved in enabling other mothers of breech-presenting babies to become involved in shaping the evolution of this research.
Birth Experience
I spoke with 7 women with a breech presentation at term and 1 doula over video calls in groups of 2. We started by sharing our breech birth experiences and the themes of lack of choice and lack of confidence in birthing professionals echoed across all interviews. The need for support towards a physiological breech birth was not met in many of the experiences resulting in a lack of choice and feelings of coercion towards a c-section. They reported a confidence in their body’s own ability to birth breech, but a lack in the birthing professional’s ability to confidently support them.
The mothers were aware of optimal cord clamping and the benefits, however, similar to the women in our OptiBreech studies, they had reported feeling let down because the cord was clamped immediately, despite stating their wishes on their birth plan. They also reported not being made informed as to why the cord was clamped immediately.
Some of the mothers also reported their baby being taken to a resuscitation table out of sight without being informed. Seeing their baby on the resuscitation table led to feelings of self-doubt, guilt and questioning whether they had made the right choices.
Is this research proposal important and relevant?
The research proposal aims to answer two questions:
What are the outcomes for mother and baby for term breech pregnancies within the services offering optibreech care?
And can bedside stabilisation and/or resuscitation following vaginal breech births be successfully implemented with provision of a bedside unit and staff training?
About 1:5 babies born after a vaginal breech birth need some help to start breathing, and about 1:10 are transferred to a neonatal intensive care unit after the birth. We feel we can reduce this to 1:5 (the UK national average for all births) if our specialist teams are able to provide help next to the mother. This will result in better long-term outcomes for the baby. Families have better experiences if they are not separated from babies, during resuscitation or after. Women in our OptiBreech studies have reported feeling let down because in most births where the baby appeared to need help, the cord was cut immediately, despite OptiBreech and UK Resuscitation Council guidance.
All mothers strongly support the research proposal and believe optimal cord clamping and keeping the baby near to them immediately post-birth is hugely important. Some mothers reported feelings of confusion as to why this did not happen in their experience because they felt it was quite obvious that babies should be near their mother immediately post-birth, therefore were supportive of having a bedside unit so that they could always see their baby if they needed resuscitating.
Mothers reported doing more research on neo-natal death rates resulting in them feeling less informed around the need for resuscitation. Sharing this scenario before birth would help to keep the mother informed around a potential post-birth scenario as well as the need to keep the mother informed in real-time should a resuscitation unit be needed.
Language
The importance of the use of language was highlighted, in particular the use of the word “resuscitation” did not resonate well with some of the mothers as it can lead to negative connotations such as not being able to breathe or death. There was an understanding that the resuscitation table is also used for clearing the lungs and or for simply checking the baby and therefore the word “resuscitation” should be carefully considered when speaking to mothers to avoid panic. “Transition” was one replacement word suggested, however, there were mixed responses to this word as some felt it wasn’t specific enough and needed explaining whereas others responded positively saying it’s a mid-way point. There will need to be further consideration around the use of language and the most appropriate terminology to use.
Thank You
We ended the session by sharing our motivation for joining this PPI meeting and learnt that mothers wanted to be a part of the driving force behind normalising physiological breech birth, and to avoid other mothers and birthing people feeling like they have no other option.
I would personally like to say a huge thank you to those who participated in this PPI meeting, it was a pleasure meeting each of you. We value your thoughts and comments to improve on the design of our study to better our research.
If you would like to offer feedback privately, you can contact our PPI Lead, Siân Davies. Siân has lived experience of breech pregnancy, is a perinatal psychologist by training, and has additional training in trauma-informed care. Our PPIE team also includes Nimisha Johnstone.
We held two online engagement events in March 2023. These were attended by four women with lived experience of breech pregnancy and planning a vaginal breech birth and two midwives. Additional feedback was obtained via social media channels and a survey. This was how we advertised them:
Monday, 6 March, 2-3.30 pm — via Zoom
Tuesday, 14 March, 6-7.30 pm — via Zoom
Events are open to women and birthing people and maternity care providers throughout the UK.
Below is a description of one of the studies we would like to do. We invite anyone to comment on the study design and description (online survey; will remain open until early May 2023), particularly families that have had a breech-presenting baby within the past 5 years in the UK. We can answer any questions you have during the engagement meetings, or you can contact us via e-mail using the form below.
OptiBreech ECV or no-ECV trial
ECV with midwives Shawn and Lucia Pederiva (shared with permission)
Approximately 1:25 babies is breech at the end of pregnancy, positioned head-up instead of head-down in the womb. Current standard care is to offer women an attempt at turning the baby to head-down, through pressure on the abdomen (external cephalic version, ECV). However, this procedure is only successful 50% of the time and some women prefer not to try it.
OptiBreech care is delivered through a dedicated clinic, co-ordinated by a breech specialist midwife collaboratively with a breech lead obstetrician. It includes care during labour for women and birthing people who plan a vaginal breech birth (VBB). In our first study of OptiBreech care, women who planned a VBB without a prior attempt at ECV (no-ECV) had higher rates of vaginal birth. In our small trial, women receiving OptiBreech care had higher rates of vaginal birth and better outcomes compared to women receiving standard care, including all modes of birth.
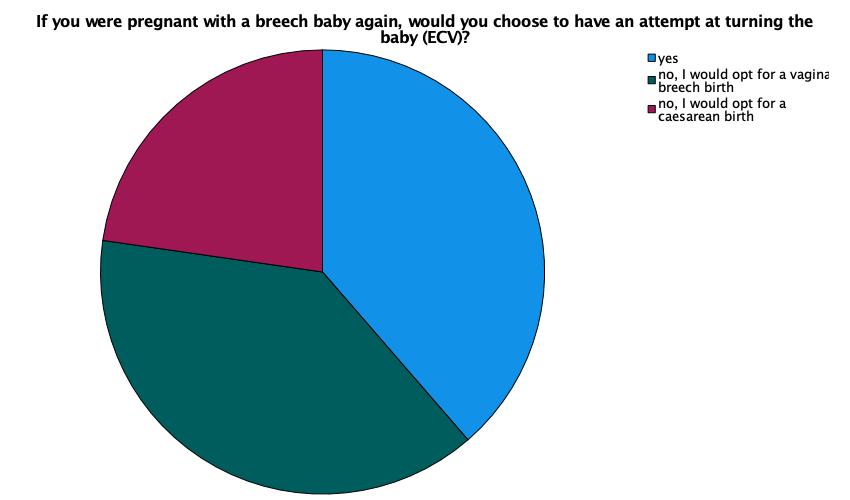
In surveys one month after birth, 60% (29/48) of OptiBreech participants said they would not attempt an ECV in a future pregnancy. OptiBreech clinicians are also uncertain whether trying to turn the baby provides additional benefits, including more vaginal birth and less overall healthcare costs, compared to no-ECV within OptiBreech services.
The thoughts of 48 women following breech pregnancies on ECV if they had another breech baby. Note: This is a current snapshot of our responses and may change. Also, more women in this sample had unsuccessful ECVs, which will influence views.
The aim of this research is to determine if attempting to turn breech babies head-down (ECV) offers additional benefits, compared to OptiBreech care with no-ECV.
The design is a randomised controlled trial. Participants will be women over 36 weeks of pregnancy who wish to plan a vaginal birth regardless of whether their baby remains in a breech position. Those who choose to participate will be allocated by chance (randomised) to one of two options.
The ‘standard care’ group (the control) will have an ECV attempt. If unsuccessful, the person will plan a VBB with OptiBreech care. The experimental group will be no-ECV; these will plan a VBB with OptiBreech care. We will compare these two groups to determine whether the vaginal birth rate differs between them and whether care for one group costs more than care for the other.
Our stakeholders, OptiBreech clinicians, participants and Patient and Public Involvement group members, have highlighted the need for this research. While some women may continue to prefer an ECV attempt, others would prefer not to have one if additional benefits are not clear. This could potentially save healthcare resources or alternatively reassure us that ECV is still important in OptiBreech contexts.
This research is aimed at influencing national guidance. We will work with the Royal College of Obstetricians and Gynaecologists to ensure this happens. We will also share our results with participants and the public through publications and our engagement website, optibreech.uk.
Dr Shawn Walker, OptiBreech Chief Investigator
Stakeholder feedback and questions
From our first engagement event:What happens if someone gets randomised into ECV and they didn’t want this and decides not to go ahead with the plan?
Ideally, we would like people to decide if they will be happy to have an ECV and/or a planned vaginal breech birth before agreeing to participate. However, we respect everyone’s autonomy and ability to withdraw from research interventions. We would continue to include the person’s results (with consent) and would take account of the change of plan in the statistical analysis. The reality of breech care is people often do change their minds, both about ECV and about VBB.
Could woman opt in for ECV or no ECV themselves?
Yes, but not if they are participating in the trial. Randomisation reduces bias by removing the element of choice from both women and clinicians. So participants would need to decide if they are happy to give up that choice, and accept ECV or no-ECV according to the way they are randomised.
If women decide NOT to participate in randomisation but still wish to plan a vaginal breech birth, they will be invited to participate in the observational cohort arm of the study. This option may or may not be available to women booked externally to participating centres, depending on whether OptiBreech care is considered the standard of care or an experimental treatment (on-study only) within that hospital. It may also depend on the team’s capacity.
From our first engagement event:If someone has had a previous caesarean birth but they would like this birth to be vaginal, could having an ECV cause issues because of the previous birth mode i.e. ruptured membranes etc?
From our first engagement event (midwife stakeholder):Computer randomisation does reduce clinical bias, however would the clinical midwife involved in the study increase bias by them recruiting participants?
Yes! This bias could go either way. Sometimes people are not recruited because, for example, the clinician does not feel it would be appropriate to offer them one option or another. Sometimes there is confusion about inclusion criteria so that women at moderate risk (eg. one previous caesarean birth) are not offered the opportunity to participate. To counter-act this potential source of bias, we will create posters for recruiting sites to display in areas where women receive antenatal care, providing them with a neutral point of contact, such as a research midwife. We will also share information on this website about how women can self-refer onto the study. This will enable as many women to access the research as possible and limit the bias from clinician selection.
From our online survey:How do people get consented to the randomisation?
Great question! The health care professional who informed the person about the research would offer further written information and the opportunity to ask questions. Then we would ask for consent, usually online, directly onto our database via the participant’s personal e-mail, which is also used for follow-up surveys. Alternatively, consent can be taken via written signature on the same consent form, on paper. An example of the participant information sheets and consent forms we currently use can be found on our Information for Women and Birthing People page.
In some settings, OptiBreech team care has become the standard of care. In others, it is still considered an experimental care pathway within the service, with the service funded by clinical research network funds. In the latter case, OptiBreech care would only be available through participation in the research.
From our online survey:I’d want more information about what OptiBreech is, but appreciate this may confound the research.
We want participants in this research to have a very clear idea about what OptiBreech Care is. We explain it in our participant information sheets, which are similar to those we would use in this research. These can be found on our Information for Women and Birthing People page.
Questions about breech birth at home
From our online survey:
What about those who wish to birth at home?
I suspect the research will take place in hospital, but that hasn’t been made clear.
Supporting women in any location.
Any data on VBB home birth.
Our OptiBreech Guideline recommends birth in hospital, within an obstetric unit. However, this is not required. We neither require women to give birth in hospital nor require local OptiBreech teams to attend births outside of the hospital. As with most standard breech criteria, our approach is to observe rather than to control. Women on our study have chosen to give birth in the full range of settings available to all other women, although sometimes the ability to do this is affected by local staffing constraints. It is too early to offer information about how place of birth influences results for OptiBreech care.
From our online survey:Does this include footling breech presentation? As all basic literature I have found suggests c section always offered with these.
You are absolutely correct that this has been the traditional approach. But our approach is to base all of our guidelines on evidence.
Our view of the literature is that ‘footling’ presentation is poorly and inconsistently defined, making it difficult to draw conclusions about risk. Increased risks pre-term (before 37 weeks) are clear, but the available literature indicates that non-extended (non-frank / both legs straight beside the body) presentations may actually have BETTER outcomes at term. We therefore do not recommend a caesarean birth unless the feet are presenting and the baby’s pelvis is not engaged, eg. positioned above the inlet to the maternal pelvis. We call this position, ‘standing.’
When baby’s legs are flexed (bent), we counsel women about the increased risk of a cord dropping down in labour, which would require a caesarean birth if it happened. And we explain the clinical uncertainty, eg. we do not know for certain whether there is increased risk or not.
Instead, we collect data about what position baby’s legs are in during antenatal scans and what position the legs are in at birth, and of course what the ultimate outcome is. In that sense, yes, footling breech presentation is included, and not excluded, from this research.
How will you record babies that turn by themselves without an attempted ECV or after a failed ECV?
In the OptiBreech database, we record: 1. Initial plan after first counselling – ECV/VBB/CB; Result of all ECVs planned – not done (and reason)/successful/unsuccessful
Will you allow a 2nd ECV after a failed ECV?
Yes, all women who request an ECV are offered a 2nd attempt (for those women randomised to the ECV arm only).
What will your approach be to other turning methods eg spinning babies, moxibustion, Webster’s technique?
In the OptiBreech database, we record: 1. Counselling, advice, information and other items (eg. moxa sticks) women have been given antenatally; 2. What women report having used in pregnancy in a follow-up survey 1 month after birth
Will women have to agree not to try them or will they be allowed or even encouraged? In either case the data on what else they try will need to be collected.
Currently, the OptiBreech care pathway does not include specific advice on complementary therapies. We are collecting observational data on their use only. We will neither be requiring women not to try complementary therapies nor encouraging them to do so.
Hope that helps! Keep up the good work!!!
Thank you!
OptiBreech is helping so many women that are coming through our group – I hope you can find a way to make it more widely adopted once the research is completed (but I realise the NHS is slow…)
We are working on that too! Watch this space …
Responses to the online survey
Who participated?
Other: I experienced undetected footling breech presentation and delivered vaginally at home prior to midwife arrival due to rapid labour. Just over 2 months ago.
Q1 – What do you like about this study?
I felt like my only option was elective c-section so this would have been great to support a vaginal breech birth for me
I am interested to know if not attempting an ECV would lead to better outcome. And how good are the outcomes for mum and baby in BVV.
Having options to birth vaginally rather than being told you must have a c section. That there will be specialists in breech aginal delivery
That it could support trusts to support VBB
The encouragement of the use of natural breech birth
The results can influence that women should not be forced into an ECV automatically. Autonomy is so important
Each study arm has an emphasis on vaginal birth; the study will collect good data on the outcomes of VBB attempts in general and this will allow more birthing people to consider a VBB, with or without ECV.
It could provide some insight to the reality of the benefit of ECV rather than a perceived benefit. Any additional information on breech birth will help empower women with their birth choices.
I like that methods other than ecv are being looked at.
Its taking a good look at optimum care for women with a breech presentation, acknowledging that they may want a vaginal birth and this is a perfectly reasonable option.
It is lookind xarefully at the impact of ECV. It is supporting vaginal breech birth
I like that women would be allowed to make an informed choice without being pressurised into what they don’t want, considering there are no further risk factors involved
It looks at the clinical benefits and outcomes of a procedure which is often just assumed, or denied without a real discussion
Providing more data on the benefits of an ECV to allow people to make informed choices
I like the idea that in one group the baby decides- if it stays breech it can be born breech. I like that both groups will get to birth vaginally
I think ECV can seem like ‘an automatic’ thing to do when your baby is breech. I think it is important to look into this into more depth as it never really has been done before. I had an ECV but if I were to have another child who presented breech I would not have one and either wait for baby to turn or go for a vaginal birth (if no contradictions)
I like that you are looking at the various options of breech babies & better outcomes. If it leads to women being able to choose to birth vaginally instead of being coerced into a c-section then I am all for it. We need more education about vaginal breech births in the NHS
It is looking to educate and empower and provide HCPs with a level of experience in delivering breech babies that is severely lacking within the NHS. Looking to inform woman that breech is normal and not in isolation, a reason for concern.
Having an ECV is very stressful, and though risk is low, safety can’t be guaranteed. If there is no additional benefit to having one, it’s potentially an unnecessary and step leading to less successful vaginal births. If safe breech vaginal delivery was normalised, women may be less scared into having an ECV
Simple design
Q2 – Did anything concern or worry you?
No
No.
No
No
no
Not really
No
Not currently.
No. But I know some women worry about ECV. I had one (which didn’t work) so I’m not bothered.
What about thoae who wish to birth at home?
No
No
No
No, I think this is well thought out research
No
That this is purely about whether or not to have an EVC. Also will it lead to yet another thing to coerce women into doing?
There is a lot of coercion within maternity care. No matter the guidelines, assurances or gaslighting that goes into denying or covering it up. I would be concerned as a mother anticipating a breech baby that when I came to labour, a medical team who did not support the trial would be charged with my care. I would be denied my birthplan. That any slowing or deviations from a classic progression and delivery would be blamed on the breech and so start the process of implanting doubt and then coercion of a woman in a vulnerable state of labour towards a section as this is the route that the clinicians feel they have the most control of the outcome.
To encourage more women to participate, they should be able to swap groups if they feel more comfortable having or not having an ECV when the time comes
I supposed if someone was randomised they took ECV and really wanted one they could opt out, or vice versa
Q3 – Was there anything you needed more information about, or felt was unclear in the summary?
Note: Where participants expressed questions, we answered these above.
No
No
No
yes
No
Very clear
Does this include footling breech presentation? As all basic literature I have found suggests c section always offered with these.
How do people get consented to the randomisation
I’d want more information about what OptiBreech is, but appreciate this may confound the research. I suspect the research will take place in hospital, but that hasn’t been made clear.
No
No
No
No, it was all clear
No
If a person has birthed before… are first time persons more likely to be reluctant to participate. Once you have experienced labour and birth are you more likely to elect for a breech? I think I would have been reluctant with my first (head down) as birth was venturing into the unknown but I personally wanted to with my second. Sadly I wasn’t given the option. My trust informed me I was either successful ECV or it had to be a section as there wasn’t anyone who would deliver a breech baby. It wasn’t until much later that I realised that I had been bullied into consenting to an unnecessary procedure and not given any time to make an informed decision.
No, very clear
Perhaps that person giving birth always has a choice about the treatment they pursue
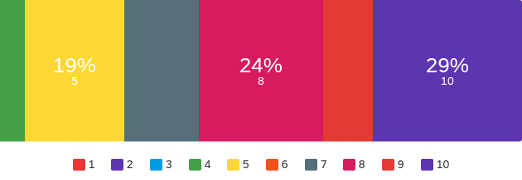
Q4. If we asked 10 women or birthing people who prefer a vaginal birth if they would like to participate in this study, how many of these 10 women do you think will agree to participate?
Minimum: 4
Maximum: 10
Mean: 7.76
Standard deviation: 1.95
Q5. If you were pregnant with a breech baby, would you participate in this study?
All 21/21 women who participated in our survey indicated they would participate in this study.
Q6 – Why do you feel this study will be acceptable, or not?
Yes
I think it’s acceptable, it’s an interesting topic
Acceptable because it gives women choices with their bodies and births which reduces trauma surrounding a lack of control to try birth vaginally
Na
yes
Anything that gives women autonomy is so important, as they have to deal with the consequences of it. You shouldn’t be made to feel that is the only option
Dedicated care for breech presentation to optimise the chances of a successful vaginal birth in both arms.
It may be tricky because VBB can be taboo, and offering ECV is a standard of care. Some women may feel they are not giving themselves the best chance if they don’t attempt an ECV
Some women won’t want to risk having an ECV.
If birthing people have strong feeling ref ECV they may withdraw if allocated to the ‘wrong’ group.
It allows women making informed choice whilst considering research data and risk factors
This is a really vulnerable time in a pregnancy. Women often have ideas about how they are going to give birth, they are often told for weeks/months don’t worry baby has lots of time to turn and then suddenly it’s all systems go for a c section. It should be talked about more throughout with real tangibility of success rates and impacts
Support of the OptiBreech team will mean candidates are more likely to support a randomised study as they will feel well cared for by experts
I’m both groups there is clearly good care and support from a breech team
It looks into the area in more depth and gives women and birthing people more information as a result
Education on babies needs to be bought to the table.
Anything to enable fewer interventions in a healthy pregnancy and labour can only be beneficial.
If I was pregnant for a second time with another breech baby I would definitely participate as I’m no longer concerned about having a breech vaginal delivery following my participation in the Optibreech trial. Had this opportunity been given to me with my recent breech pregnancy, I would have preferred to have a choice as to which group I was allocated as I wanted to try and turn my baby. If safe breech vaginal deliveries were normalised and it was well known that having a breech team meant a safer delivery than all modes of birth, I think I would have been relaxed about whether to have an ECV or not and therefore willing to participate in either group.
Not a very high risk procedure. Painful though
Q7 – Is there anything else you would like us to prioritise for OptiBreech research?
Further expanding OptiBreech sites/upskilling more midwives and HCP so more women and birthing people have a real choice
I would like to learn more about the outcomes of the VBB when attempted with help of an experienced team.
The collection of evidence to support VBB and VBac
Could woman opt in for ECV or no ECV themselves?
Any data on VBB home birth.
Supporting women in any location.
Getting all hospitals to offer real choice to pregnant women
Yes – educating healthcare workers that breech is ‘normal’ – not a disaster waiting to happen.
It would be interesting to know if labour during breech vaginal deliveries is quicker than head down.. I think I read somewhere that it is? With regards to labouring at home and knowing how soon you should go into hospital. Should women labouring with a breech baby be encouraged to attend hospital sooner than head down.
Na
We also asked for permission to include the quotes provided in our report. Thank you to all those who have helped us to shape this research and our on-going projects.